
La hemorragia subaracnoidea (HSA) es una de las urgencias neuroquirúrgicas más frecuentes, siendo la ruptura de un aneurisma intracraneal la principal causa. La hidrocefalia es una complicación neurológica prevalente y presenta una elevada tasa de complicaciones y necesidad de reintervenciones. Los objetivos de este trabajo son identificar los factores predictores de la colocación de derivación ventriculoperitoneal y conocer la tasa de complicaciones asociadas a estos dispositivos en nuestro centro. Con ello, se pretende seleccionar a los pacientes que requieren la colocación temprana de una derivación con el objetivo de reducir las complicaciones.
Material y métodoSe trata de un estudio observacional retrospectivo analítico de los pacientes con HSA espontánea derivados al Hospital Universitario Miguel Servet de Zaragoza entre 2017 y 2022. Se han recogido diversas variables como características clínicas y radiológicas, tipo de tratamiento, diagnóstico y terapia de la hidrocefalia, tiempo hasta la colocación de la derivación ventriculoperitoneal (DVP), complicaciones de la DVP y mortalidad global de la HSA. Se ha realizado un análisis estadístico para comprobar si existe asociación entre estas variables y la necesidad de colocación de la válvula. Posteriormente se comparan los resultados obtenidos con los existentes en la literatura. Este estudio ha sido aprobado por el Comité de Ética de Investigación Clínica de Aragón (CEICA).
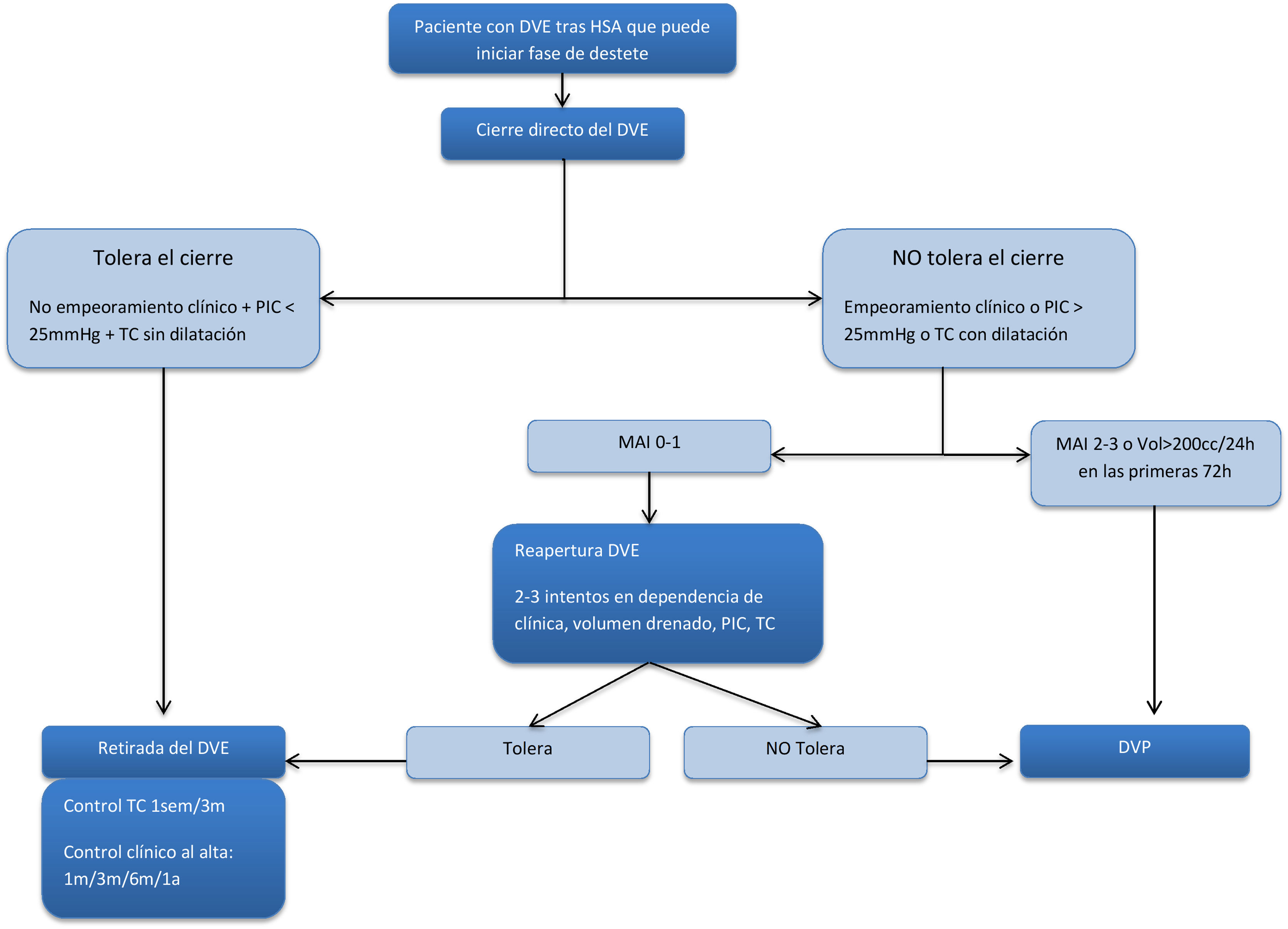
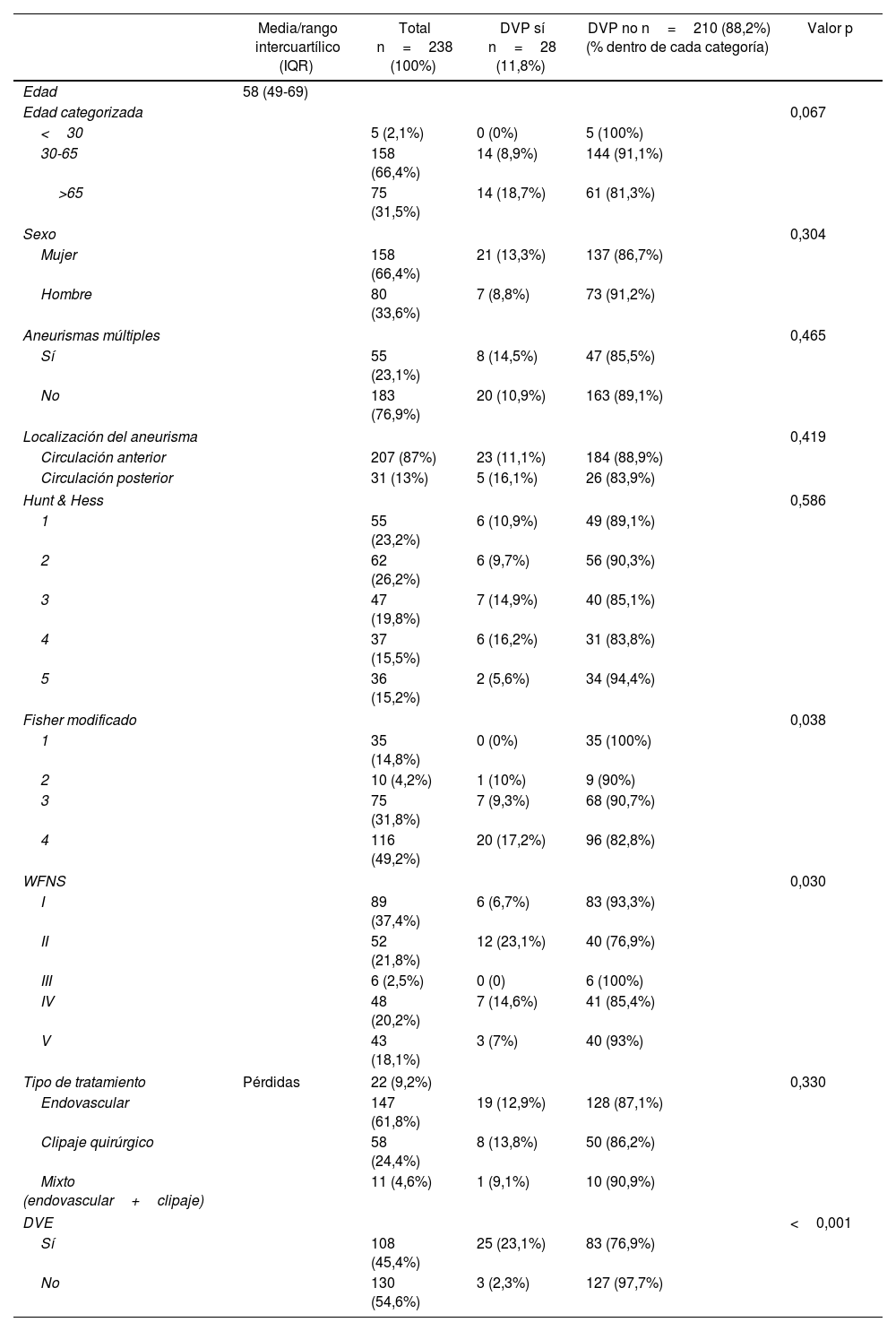
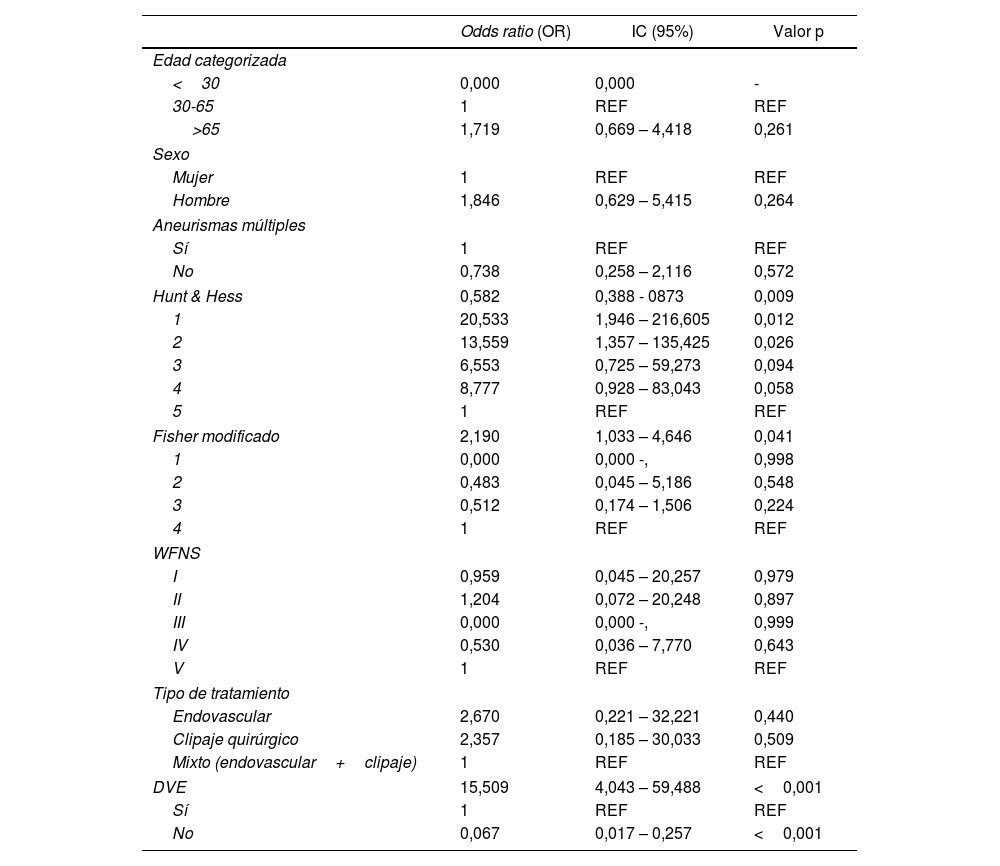
ResultadosEntre 2017 y 2022 se recogieron un total de 359 personas con HSA espontánea derivados a nuestro centro, presentando una mortalidad intrahospitalaria de 25,3%. De las HSA, 66,3% (n=238) fueron secundarias a la ruptura de un aneurisma. De los pacientes, 45,3% con HSA aneurismática requirieron la colocación de un drenaje ventricular externo (DVE) y 11,7% (n=28) necesitaron la colocación de una DVP por hidrocefalia permanente. Existe relación estadística entre la colocación de DVP y una puntuación alta en la escala de Fisher modificada y la colocación previa de DVE. El tiempo medio hasta la colocación de la DVP fue de 26,1 días, encontrándose diferencias significativas entre el tiempo de DVE y la infección del mismo, pero no con la infección de la derivación definitiva. La tasa de reintervención de las válvulas fue de 17,7%, principalmente por infección del sistema.
ConclusionesLos factores de riesgo que permiten predecir la colocación de DVP son una puntuación alta en la escala de Fisher modificada y la colocación previa de DVE. La infección valvular es la complicación más frecuentemente asociada a reintervención quirúrgica. Consideramos que una actitud más proactiva a la hora de la colocación de DVP en estos pacientes podría disminuir la tasa de complicaciones.
Subarachnoid hemorrhage (SAH) is one of the most frequent neurosurgical emergencies, most of them due to intracranial aneurysm rupture. Hydrocephalus is a prevalent complication with a high rate of complications. The aims of this study are to identify predictors of shunt-dependent hydrocephalus following aneurysmal SAH and to quantify the complications arising from ventriculoperitoneal shunts.
Material and methodsThis study is about an observational retrospective analytic study of the patients with spontaneous SAH admitted to Miguel Servet Universitary Hospital between 2017 and 2022. Patients’ clinical and radiological characteristics, type of treatment, diagnoses and treatment of hydrocephalus, complications of ventriculoperitoneal shunts and mortality are some of the data achieved in this study. A descriptive study of these variables has been done and, subsequently, the most relevant variables have been statistically analyzed to identify patients with increasing risk of shunting for hydrocephalus. This study was authorized by the Ethics Committee prior to its elaboration.
ResultsA total of 359 patients with spontaneous SAH were admitted to Miguel Servet Universitary Hospital between 2017 and 2022, with an intrahospitalary death rate of 25,3%. 66,3% of the total of patients with SAH were due to intracranial aneurysm rupture (n=238). 45,3% of the patients with aneurysmal SAH required an external ventricular drain (EVD) to treat acute hydrocephalus. 11,7% (n=28) developed a shunt-dependent hydrocephalus. Statistical significance was found between shunt-dependent hydrocephalus and the following: high score in modified Fisher scale and placement of EVD. The mean interval from EVD to ventriculoperitoneal shunt placement was 26,1 days. The mean rate of reoperation of patients after shunt was 17,7%, mostly due to infection.
ConclusionsThe most significant risk factor for shunt-dependent hydrocephalus after aneurysmal SAH was high Fisher grade and previous need of EVD. Shunt infections is the main cause of shunt reoperation. Early shunt placement in selected patients might reduce the rate of infectious complications.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.