
To analyze the primary complications related to semisitting position in patients undergoing cerebelo-pontine angle surgery.
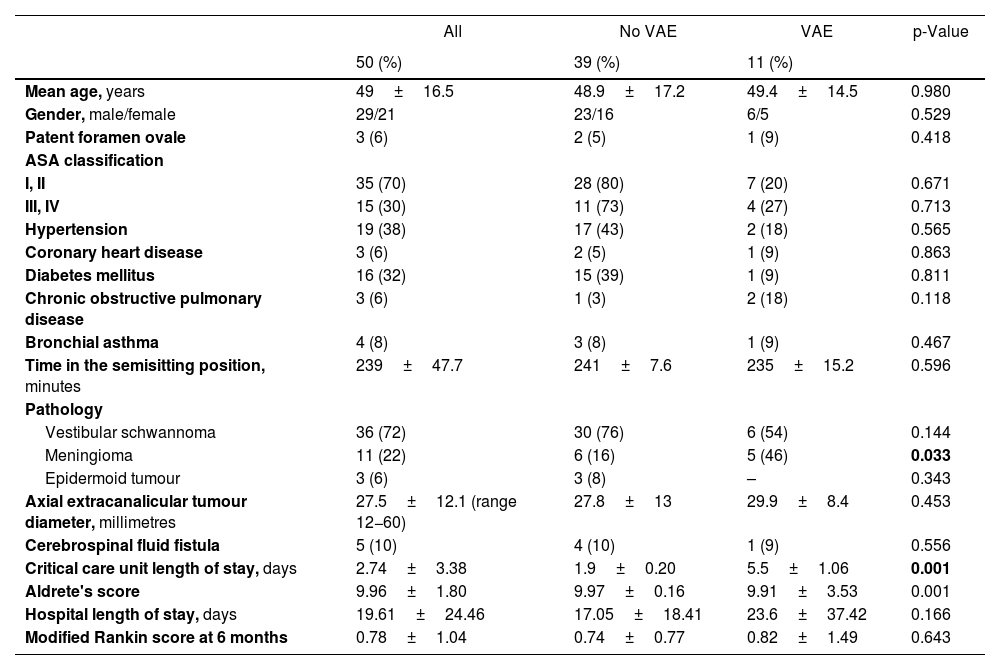
MethodsRetrospective data analysis from patients undergoing elective tumoral cerebelo-pontine angle surgery in a semisitting position. The incidence, severity, occurrence moment, treatment, duration, and outcomes of venous air embolism (VAE), pneumocephalus, postural hypotension, and other complications were recorded. Neurointensive care unit (NICU), length of stay (LOS), hospital LOS, and modified Rankin scale scores were calculated six months after surgery.
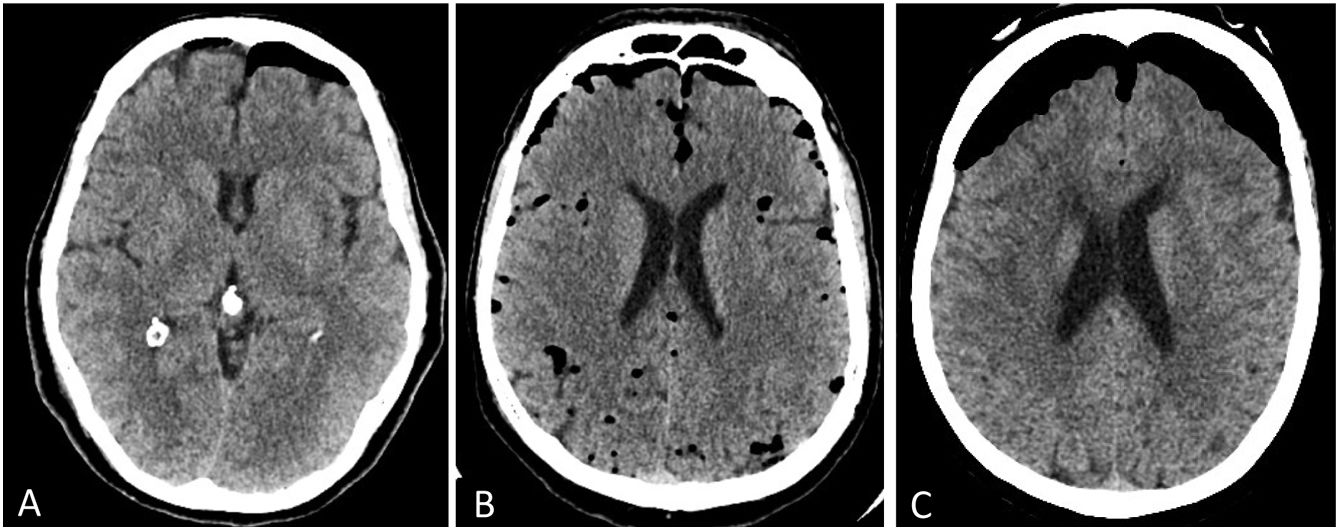
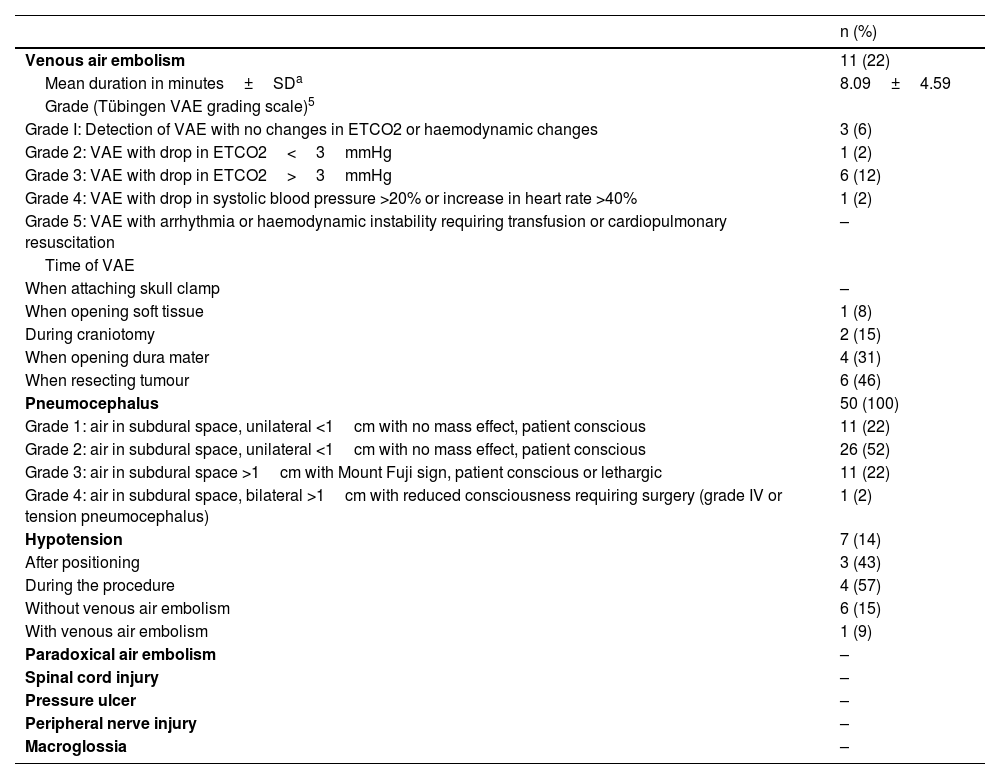
ResultsFifty patients were operated on. Eleven (22%) presented VAE (mean duration 8±4.5min): five (10%) during tumor resection, and four (8%) during dural opening. Ten (20%) were resolved by covering the surgical bed, air bubbles aspiration, jugular compression, and one (2%) tilted to a steep Trendelenburg position. One (2%) had intraoperative hemodynamic instability. The only variable associated with VAE was meningioma at histopathology OR=4.58, p=0.001. NICU was higher in patients with VAE (5.5±1.06 vs. 1.9±0.20 days, p=0.01). There were no differences in the Rankin scale. All patients presented postoperative pneumocephalus with a good level of consciousness, except one (2%) who required evacuation. Seven patients (14%) showed postural hypotension, three (6%) after positioning, and one (2%) after developing a VAE; all were reversed with usual vasoactive drugs. No other position-related complications or mortality were registered in this series.
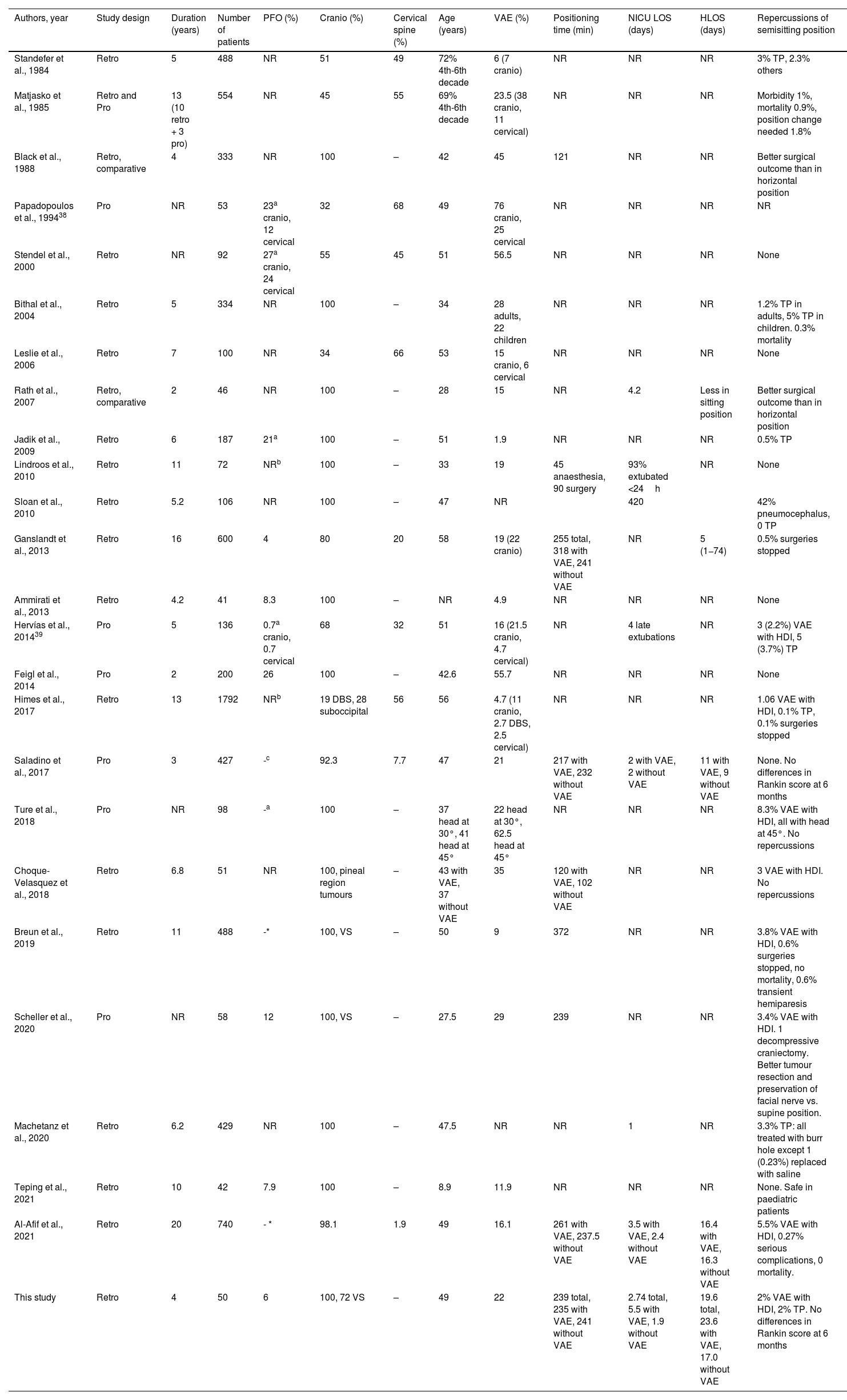
ConclusionsThe semisitting position is a safe option with the knowledge, prevention, detection, and early solution of all the possible complications. The development of VAE rarely implies hemodynamic instability or greater disability after surgery. Postoperative pneumocephalus is very common and rarely requires evacuation. Excellent cooperation between anesthesia, nursing, neurophysiology, and neurosurgery teams is essential to manage complications.
Analizar las complicaciones asociadas a la posición semisentada en pacientes intervenidos de patología del ángulo pontocerebeloso (APC).
MétodosEstudio retrospectivo, se analizaron los pacientes operados de patología tumoral del APC por un abordaje retrosigmoideo en posición semisentada. Se analizó la incidencia, gravedad, momento de aparición, forma de resolución, duración y repercusiones del embolismo aéreo venoso (EAV), neumoencéfalo, hipotensión postural y otras complicaciones. Se analizó el tiempo de estancia en unidad de críticos (TUCRI), tiempo de estancia hospitalaria (TEH) y puntuación en escala de Rankin a los seis meses.
ResultadosSe intervinieron 50 pacientes, once (22%) presentaron EAV (8±4,5 minutos duración media): cinco (10%) durante la resección tumoral, cuatro (8%) durante la apertura dural. Diez (20%) se resolvieron tapando el lecho quirúrgico, aspirando burbujas y aplicando compresión de yugulares, uno (2%) requirió cambio de posición. Uno (2%) tuvo repercusión hemodinámica intraoperatoria. La única variable asociada con desarrollar EAV fue una anatomía patológica de meningioma OR=4,58, p=0,001. El TUCRI fue superior en pacientes con EAV (5,5±1,06 vs. 1,9±0,20 días, p=0,01). No hubo diferencias en la escala Rankin. Todos presentaron neumoencéfalo posquirúrgico con buen nivel de consciencia, salvo uno (2%) que requirió de evacuación. Siete pacientes (14%) presentaron una hipotensión arterial, tres (6%) tras la colocación y uno (2%) tras un EAV, todos revertieron con vasoactivos. No se registraron otras complicaciones asociadas a la posición ni mortalidad en esta serie.
ConclusionesLa posición semisentada es segura si se conocen, previenen, detectan y solucionan precozmente sus posibles complicaciones. El desarrollo de EAV rara vez implica repercusión hemodinámica intraoperatoria ni mayor discapacidad a los seis meses. La aparición de neumoencéfalo es la norma, siendo excepcional que sea a tensión y requiera de evacuación. Para ello es imprescindible una excelente cooperación entre el equipo de anestesia, enfermería, neurofisiología y neurocirugía.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.