



The coronavirus disease 2019 (COVID-19) has amazed by its distinct forms of presentation and severity.
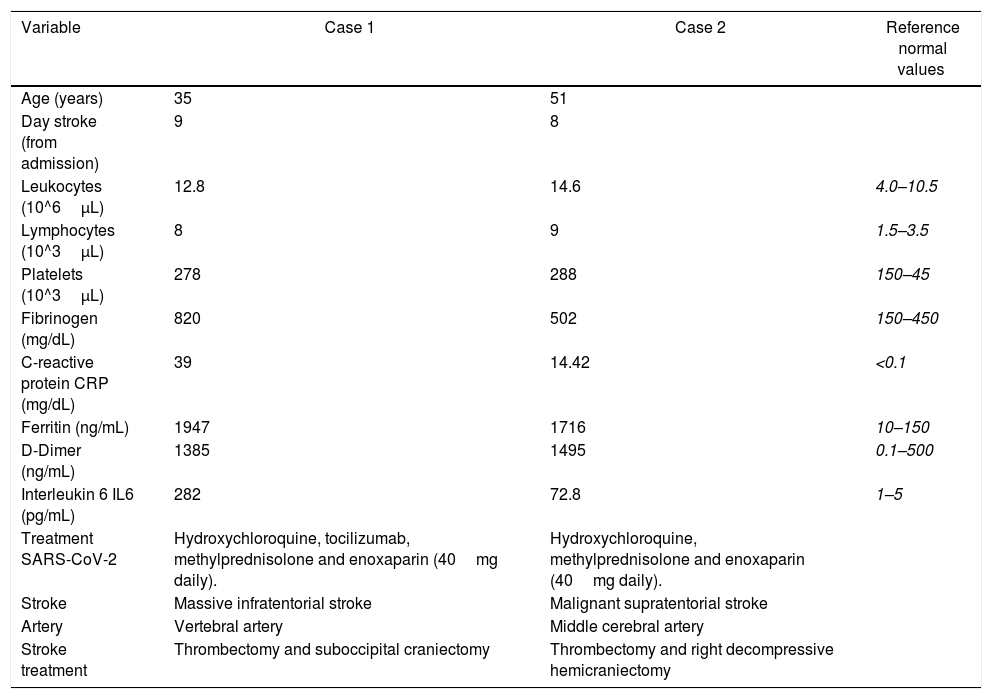
COVID-19 patients can develop large-scale ischemic strokes in previously healthy patients without risk factors, especially in patients who develop an acute respiratory distress syndrome (SARS-CoV-2).
We hypothesize that ischemic events are usually the result of the combined process of a pro-inflammatory and pro-coagulant state plus vascular endothelial dysfunction probably potentiated by hypoxia, hemodynamic instability, and immobilization, as reported in other cases.
To the best of our knowledge, we report the first case of partial obstruction of a vertebral artery in a patient with COVID-19.
Decompressive surgery remains a life-saving maneuver in these patients (as in other non-COVID-19 strokes) and requires further investigation.
La enfermedad por coronavirus 2019 (COVID-19) ha sorprendido por sus distintas formas de presentación y gravedad.
Los pacientes con COVID-19 pueden desarrollar accidentes cerebrovasculares isquémicos a gran escala, incluso aquellos previamente sanos, sin factores de riesgo, y especialmente los que desarrollan un síndrome de dificultad respiratoria aguda (SARS-CoV-2).
Presumimos que los eventos isquémicos son generalmente el resultado del proceso combinado de un estado proinflamatorio y procoagulante, más una posible disfunción endotelial vascular, probablemente potenciada por hipoxia, inestabilidad hemodinámica e inmovilización, como se ha reportado en otros casos.
Hasta nuestro conocimiento reportamos el primer caso de una obstrucción parcial de una arteria vertebral en un paciente con COVID-19.
La cirugía descompresiva sigue siendo una maniobra que salva vidas (como en otros accidentes cerebrovasculares que no están relacionados con la COVID-19) y requiere más investigación.
Artículo
![]()
Si es la primera vez que accede a la web puede obtener sus claves de acceso poniéndose en contacto con Elsevier España en suscripciones@elsevier.com o a través de su teléfono de Atención al Cliente 902 88 87 40 si llama desde territorio español o del +34 932 418 800 (de 9 a 18h., GMT + 1) si lo hace desde el extranjero.
Si ya tiene sus datos de acceso, clique aquí.
Si olvidó su clave de acceso puede recuperarla clicando aquí y seleccionando la opción "He olvidado mi contraseña".




