








Magerl’s technique remains a widely accepted method for achieving C1-C2 fusion. Although two approaches using intermuscular corridors and biplanar X-ray guidance have been reported, there are no published studies dedicated to fully percutaneous techniques employing cannulated screws.
ObjectiveTo demonstrate the feasibility of a fully percutaneous C1-C2 fixation technique using cannulated screws and to analyze the short- and long-term outcomes of the initial case series.
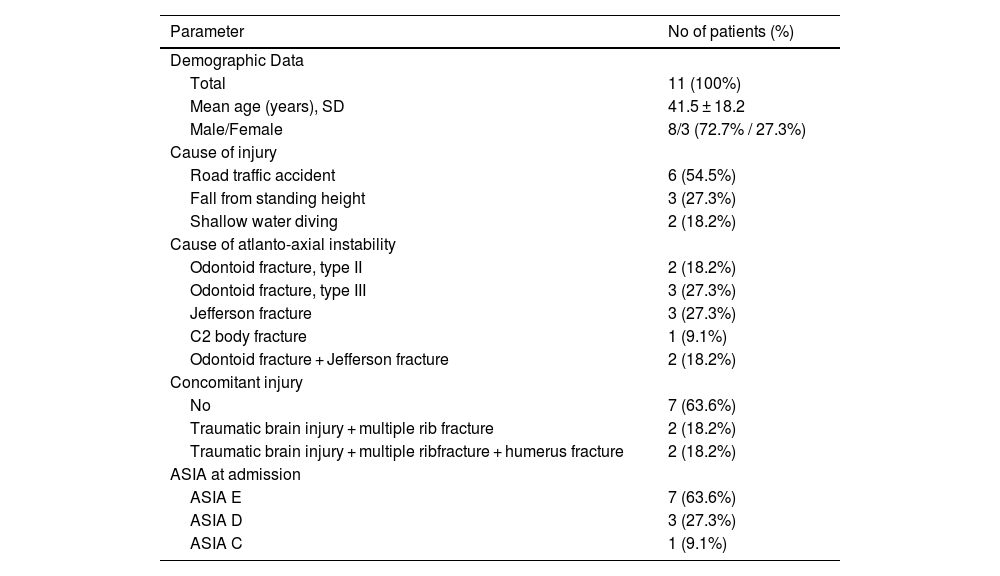
Material and methodsThis case series included patients over 15 years of age who were presented with acute or subacute atlantoaxial instability at C1-C2 due to fractures of the odontoid process, C1 vertebra, or C2 vertebral body. Surgical details and fusion criteria were described. Due to the absence of comparison groups, only descriptive statistical methods were employed.
ResultsA total of 11 patients (8 men, 3 women; mean age 41.5 ± 18.2 years) underwent fully percutaneous transarticular C1-C2 fixation. The mean operative time was 115.0 ± 30.8 min for patients stabilized using a Halo device and 80.6 ± 33.2 min for those immobilized with a Mayfield clamp. The mean blood loss across all cases was 38.8 ± 8.7 mL. One patient died from concurrent cardiac pathology. Two patients were lost to follow-up due to relocation, leaving 8 patients for final assessment. At final follow-up, the mean VAS score was 2 ± 1.5 and the mean NDI score was 5.3 ± 5.2. All patients with preoperative neurological deficits improved by one level on the ASIA scale. Fusion was achieved in 7 of 8 cases (87.5%), and 1 patient (12.5%) developed a stable C1-C2 pseudoarthrosis.
ConclusionOur initial clinical experience demonstrated that fully percutaneous posterior transarticular C1-C2 stand-alone screw fixation using cannulated instruments could be a feasible and safe procedure. Critical requirements for this technique include complete reduction of atlantoaxial dislocation, compression in the lateral joint region, adequate intraoperative visualization, and strict adherence to specific screw trajectories.
La técnica de Magerl sigue siendo un método ampliamente aceptado para lograr la fusión C1-C2. Aunque se han descrito dos enfoques que emplean corredores intermusculares y guía radiológica biplanar, no existen estudios publicados que analicen técnicas completamente percutáneas utilizando tornillos canulados.
ObjetivoDemostrar la viabilidad de una técnica de fijación C1-C2 completamente percutánea mediante tornillos canulados y analizar los resultados a corto y largo plazo de la serie inicial de casos.
Material y métodosEsta serie de casos incluyó pacientes mayores de 15 años con inestabilidad atlantoaxoidea aguda o subaguda en C1-C2 debido a fracturas del proceso odontoides, vértebra C1 o cuerpo vertebral C2. Se describieron los detalles quirúrgicos y los criterios de fusión. Debido a la ausencia de grupos comparativos, solo se emplearon métodos estadísticos descriptivos.
ResultadosUn total de 11 pacientes (8 hombres, 3 mujeres; edad media 41,5 ± 18,2 años) fueron sometidos a fijación transarticular C1-C2 completamente percutánea. El tiempo operatorio medio fue de 115,0 ± 30,8 minutos en pacientes estabilizados con un dispositivo Halo y de 80,6 ± 33,2 minutos en aquellos inmovilizados con una abrazadera Mayfield. La pérdida sanguínea media en todos los casos fue de 38,8 ± 8,7 mL. Un paciente falleció debido a una patología cardíaca concurrente. Dos pacientes se perdieron en el seguimiento debido a cambio de residencia, dejando 8 pacientes para la evaluación final. En el seguimiento final, la puntuación media de EVA fue de 2 ± 1,5 y la puntuación media de NDI fue de 5,3 ± 5,2. Todos los pacientes con déficits neurológicos preoperatorios mejoraron un nivel en la escala ASIA. La fusión se logró en 7 de 8 casos (87,5%) y 1 paciente (12,5%) desarrolló una pseudoartrosis estable.
ConclusiónNuestra experiencia clínica inicial demostró que la fijación posterior transarticular C1-C2 completamente percutánea mediante tornillos canulados es un procedimiento viable y seguro. Los requisitos críticos para esta técnica incluyen una reducción completa de la luxación atlantoaxoidea, compresión en la región de la articulación lateral, adecuada visualización intraoperatoria y el cumplimiento estricto de las trayectorias específicas de los tornillos.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



