





Peripheral nerves can present anastomoses at different levels, with intraspinal anastomoses being relatively common, but little studied.
ObjectiveTo study the presence and number of intradural anastomoses of the cervical spinal nerves in the Latin population.
Materials and methods14 adult corpses of both sexes were dissected, fixed in formaldehyde solution. Sex of the corpse, existence of anastomosis, side, height of the anastomoses and sensory/motor origin were recorded.
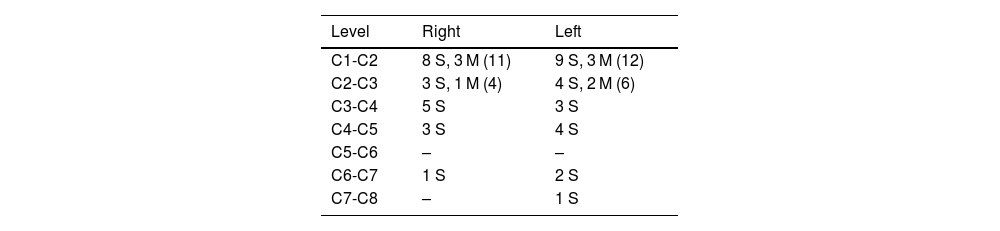
Resultsof the 14 corpses, 8 were male and 6 were female. Eleven cases presented anastomoses (79%), 8 of them bilaterally. In the total number of corpses, 52 anastomoses were found, 43 were between sensory roots (83%) and 9 between motor roots (17%). The levels where anastomoses were found most frequently were C1-C2 and C2-C3 (63% of the total).
Discussion and conclusionsintraspinal anastomoses between motor or sensory nerves can vary the clinical presentation of spinal cord injuries, radicular or medullar compressions, brachial plexus lesions or nerve root tumors, because the sensory or motor information of a given spinal cord level may be exiting the neuraxis with the adjacent spinal nerve.
Los nervios periféricos pueden presentar anastomosis a diferentes niveles, siendo las anastomosis intrarraquídeas relativamente frecuentes, pero poco estudiadas.
ObjetivoEstudiar la presencia y número de anastomosis intradurales de los nervios raquídeos cervicales en población latina.
Materiales y métodosSe disecaron 14 cadáveres adultos de ambos sexos, fijados en solución de formaldehído. Se registró sexo del cadáver, existencia de anastomosis, lado, altura de las anastomosis y origen sensitivo/motor.
ResultadosDe los 14 cadáveres, 8 fueron de sexo masculino y 6 de sexo femenino. Once casos presentaron anastomosis (79%), 8 de ellos de forma bilateral. En el total de cadáveres se encontraron 52 anastomosis, 43 fueron entre raíces sensitivas (83%) y 9 entre raíces motoras (17%). Los niveles en donde se encontraron anastomosis con mayor frecuencia fueron C1-C2 y C2-C3 (63% del total).
Discusión y conclusionesLas anastomosis intrarraquídeas entre nervios motores o sensitivos pueden hacer variar la presentación clínica de secciones medulares, radiculopatías o mielopatías compresivas, lesiones de plexo braquial o tumores de las raíces nerviosas. Esto se debe a que la información sensitiva o motora de un nivel medular dado, puede ser salir del neuroeje con el nervio raquídeo adyacente.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



