

Handedness is an epiphenomenon of brain lateralization which has been researched in the context of surgical performance, yet the same does not hold true for lateralization at a more fundamental level. We aimed to investigate whether neurosurgeons are biased in visualizing and depicting anatomy and pathology.
MethodsThis was a two part study consisting of an online survey and image analysis. An online questionnaire was used to collect basic sociodemographic data and prompt subjects to visualize surgical approaches and pathological entities and report on the side of the visualized topics. Prominent neurosurgical literature was screened for depictions of the same entities and approaches and the depicted side was noted.
ResultsThere were 49 responses, most from Croatia (n = 26), men (n = 38), right-handed (n = 42), of average age 37 years, and with 9 years of neurosurgical experience. Ambidexterity was more prevalent than in the general population. The respondents imagined the right side more commonly in all cranial-related questions, and the left side in spine-related questions. Images in neurosurgical literature showed correspondingly biased laterality.
ConclusionThere is a significant bias among neurosurgeons in laterality in processing topographical information on anatomy and pathology. Research is warranted to investigate the causes and real life implications of this phenomenon.
La lateralidad es un epifenómeno de la dominancia cerebral que se ha investigado en el contexto del ejercicio quirúrgico, pero no en un nivel más elemental. Nuestro objetivo fue investigar si los neurocirujanos están condicionados cuando visualizan y representan la anatomía y las distintas patologías que la afectan.
MétodosEstudio en dos fases que consistió, primero, en una encuesta on-line seguido de un análisis de imágenes. Se utilizó un cuestionario para recopilar datos sociodemográficos básicos y pedir a los sujetos que visualizaran abordajes quirúrgicos y entidades patológicas e informaran sobre los elementos visualizados. Además, se analizó literatura neuroquirúrgica destacada en busca de representaciones de las mismas entidades y abordajes y se anotó el lado representado.
ResultadosHubo 49 participantes, en su mayoría de Croacia (n = 26), hombres (n = 38), diestros (n = 42), con una edad promedio de 37 años y con 9 años de experiencia neuroquirúrgica. La proporción de ambidiestros fue mayor que en la población general. Los encuestados imaginaron el lado derecho con mayor frecuencia en todas las preguntas relacionadas con el cráneo y el lado izquierdo en las preguntas relacionadas con la columna. Las imágenes en la literatura neuroquirúrgica mostraron una lateralidad igualmente sesgada.
ConclusiónExiste un sesgo significativo entre los neurocirujanos en la lateralidad del procesamiento de información topográfica sobre anatomía y patología. Se precisan estudios más extensivos para investigar las causas y las implicaciones en la vida real de este fenómeno.
Most humans, neurosurgeons included, have a strong preference towards using one hand, usually the right, over the other. The phenomenon is called handedness and is widely researched topic across various fields, from genetics to cultural studies, and was shown to be associated with performance in sports, music, surgery, and road traffic safety.1–3 In neurosurgery the issue is of concern since curricula can be accommodated to overcome such innate biases and indeed it seems that the modern technological circumstances are dictating such interventions.4,5 Handedness in itself is an epiphenomenon of brain lateralization, i.e. lateralization of information processing and a special case of the general principle of functional organization observed in vertebrates.6
Even though handedness in surgery has been investigated to an extent, the same does not hold for lateralization at a more fundamental level. Namely, it is plausible that surgeons might be biased in conceptual thinking and favoring one side over the other even outside the operating theatre. This in turn might be related to a similar bias in neurosurgical training, including didactic and scholarly content, and, ultimately, patient outcomes. Such a bias we have noticed in our day to day practice, yet we failed to find any research on the topic.
Therefore we aimed to investigate the hypothesis that there exists a bias among neurosurgeons in visualizing anatomical and pathological laterality and also that the same bias is present in the neurosurgical literature.
Subjects and methodsThis was a two part study consisting of an online survey and analysis of the neurosurgical literature. The study was conducted between September and December 2023, at the Department of Neurosurgery, Clinical Hospital Center Zagreb, Croatia.
SurveyA 12-item survey form was designed in Google Forms. The questionnaire was accompanied by an introductory note to inform on the aims of the survey and sent to a pilot group of five neurosurgeons and neurosurgical residents who were asked to provide feedback on intelligibility and validity. The form was revised in accordance with the received feedback and then sent to colleagues in Croatia and abroad via e-mail. The questionnaire was constructed to collect basic sociodemographic data (sex, age, years of neurosurgical experience, professional status — resident or attending, country of residence) and data on handedness. Next, the subjects were prompted to visualize three surgical approaches (pterional craniotomy, retromastoid craniotomy, interlaminectomy) and then answer on which side was the imagined approach. This was followed by three prompts related to pathology (middle cerebral artery aneurysm, vestibular Schwannoma, herniated lumbar disc). The goal was to collect 50 responses.
Neurosurgical literature analysisTo analyze the laterality in the images in the neurosurgical literature a consensus was reached to analyze the most prominent neurosurgical atlas, textbook, handbook, and images available online. Therefore, analyzed were the Rhoton Cranial Anatomy and Surgical Approaches, Youmans & Winn neurological surgery, and the first 20 image search results on Google.7–9 The hard copies were screened for all images pertaining to any of the aforementioned anatomy or pathology. Included were all images depicting anatomy/pathology exclusively on one side and images depicting both sides, yet clearly highlighting the anatomy/pathology of a single side, until 20 were identified in total. Any ambiguities were discussed among researchers and a consensus reached on inclusion or exclusion for individual images.
Statistical analysisNominal variables were summarized as absolute (relative) frequencies, continuous variables as mean (standard deviation). Distributions of nominal variables were analyzed using the Chi-square goodness of fit test, under the assumption of equal distribution of expected outcomes. Tests were two-sided and the level of significance was set a P < 0.05. SPSS software (version 26.0, SPSS, Inc.) was used for analysis.
ResultsIn total, 49 subjects responded to the survey, of which the majority (n = 26) were from Croatia. Mean age was 37.1 ± 6.8 years, duration of neurosurgical experience 8.8 ± 6.3 years. The majority were men (n = 38), and there were more attending neurosurgeons (n = 27) than residents (n = 22). Right handedness was most common (n = 42), followed by ambidexterity (n = 5), and left handedness (n = 2). Sociodemographic data are summarized in Table 1.
Subject characteristics.
| µ/n | SD/% | ||
|---|---|---|---|
| Age | 37.1 | 6.8 | |
| Neurosurgical experience | 8.8 | 6.3 | |
| Gender (F/M) | 11/38 | 22.4/77.6 | |
| Resident/attending | 22/27 | 44.9/55.1 | |
| Handedness (left/right/ambidextrous) | 2/42/5 | 4.1/85.7/10.2 | |
| Country | Croatia | 26 | 53.1 |
| Bosnia and Herzegovina | 4 | 8.2 | |
| Czech Republic | 2 | 4.1 | |
| United States of America | 2 | 4.1 | |
| United Kingdom | 1 | 2 | |
| Nigeria | 7 | 14.3 | |
| Lebanon | 1 | 2 | |
| Italy | 4 | 8.2 | |
| Germany | 2 | 4.1 |
When prompted to visualize anatomy or pathology, the respondents imagined the right side more commonly in all cranial-related questions, and the left side in spine-related questions. The distributions of observed answers differed significantly against the assumption of equal distribution in three of the cranial-related questions, and neither of the spine-related questions (Table 2).
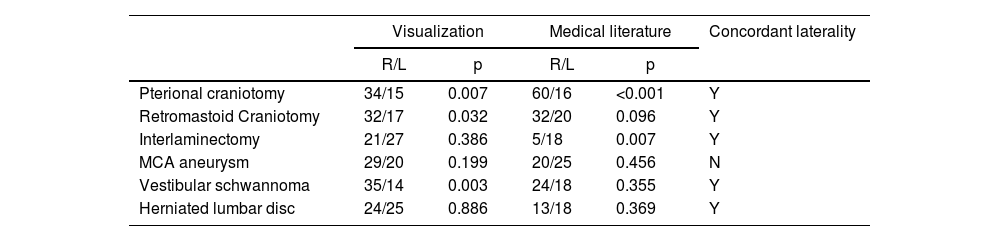
Comparison of dominant laterality in visualization and medical literature.
| Visualization | Medical literature | Concordant laterality | |||
|---|---|---|---|---|---|
| R/L | p | R/L | p | ||
| Pterional craniotomy | 34/15 | 0.007 | 60/16 | <0.001 | Y |
| Retromastoid Craniotomy | 32/17 | 0.032 | 32/20 | 0.096 | Y |
| Interlaminectomy | 21/27 | 0.386 | 5/18 | 0.007 | Y |
| MCA aneurysm | 29/20 | 0.199 | 20/25 | 0.456 | N |
| Vestibular schwannoma | 35/14 | 0.003 | 24/18 | 0.355 | Y |
| Herniated lumbar disc | 24/25 | 0.886 | 13/18 | 0.369 | Y |
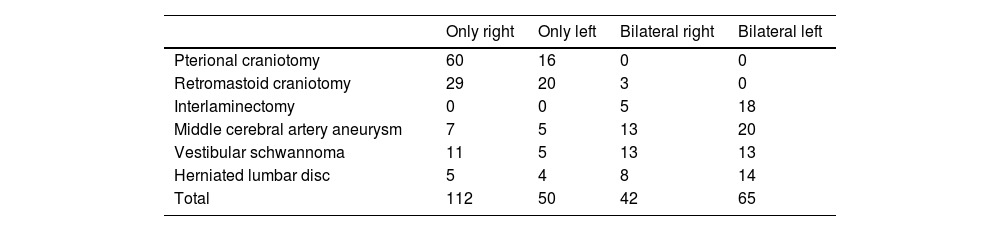
Analysis of laterality in the images in neurosurgical literature showed correspondingly biased laterality in all categories except the “middle cerebral artery” (more commonly depicted on the left in the medical literature, albeit not significantly) (Table 2). Breakdown of the analysis showed that craniotomies were depicted almost exclusively unilaterally, predominantly on the right, while interlaminectomies were depicted more commonly on the left, consistently on images showing both sides. Pathology was depicted more commonly on images that show both sides and highlight the pathology on the left (Table 3).
Laterality in images in the neurosurgical literature.
| Only right | Only left | Bilateral right | Bilateral left | |
|---|---|---|---|---|
| Pterional craniotomy | 60 | 16 | 0 | 0 |
| Retromastoid craniotomy | 29 | 20 | 3 | 0 |
| Interlaminectomy | 0 | 0 | 5 | 18 |
| Middle cerebral artery aneurysm | 7 | 5 | 13 | 20 |
| Vestibular schwannoma | 11 | 5 | 13 | 13 |
| Herniated lumbar disc | 5 | 4 | 8 | 14 |
| Total | 112 | 50 | 42 | 65 |
Our results show that neurosurgeons are biased with regard to laterality when processing information on anatomy and pathology. The bias is revealed when neurosurgeons are prompted to imagine a hypothetical case and is also reflected in how anatomy and pathology is depicted in the neurosurgical literature.
We conducted our survey on a convenient sample which was mostly from Croatia and had a higher proportion of men (77.6%), yet this proportion was lower than expected, given the results of recent studies reporting significantly higher numbers.10 We believe this to be associated with a relatively young age of our subjects, which is a generation cognizant of the importance of inclusivity and diversity.11 Owing also to young age, the resident-to-attending ratio was roughly equal.
A somewhat unexpected result was observed with regard to prevalence of non-right handedness, as the proportion of ambidextrous neurosurgeons in our sample was significantly higher than in the general population.12 However, this finding is consistent with earlier research that has shown that left-handedness and ambidexterity are more common among neurosurgeons and was even suggested that it might harbor benefits.13 Moreover, it seems likely that the (neuro)surgical ambidexterity is a an acquired feature, rather than an innate ability and can be trained, to an extent, in both right and left handed surgeons.1
We noticed several patterns in the lateralization bias in both visualization and medical literature. First, there is a significant bias toward the right side when imagining cranial anatomy or pathology and no side preference when imagining spinal anatomy or pathology. The findings are concordant in the medical literature, with the exception of the middle cerebral artery aneurysm (more commonly visualized on the right side, albeit not significantly, and no clear side preference in the medical literature). The seemingly outlying entity of the middle cerebral artery aneurysm might be explained by the fact that it is closer to the midline in the actual anatomy than the pterional craniotomy and is as such more comparable to spinal entities and perceived as “belonging to midline”. Having this in mind, we hypothesize a general law that there exists a bias toward visualizing and depicting anatomy and pathology on the right side if the actual entity is away from the midline, and the more closer the entity is to the midline, the less this bias is expressed. The nature of the concordance of the visualization and depiction bias remains to be investigated. Two alternate hypotheses are plausible: there is an underlying innate propensity to process visual information in such a biased way and both visualization and depiction are manifestations of the same phenomenon, or visualization bias is due to an artificially induced bias (via depictions in the medical literature, which in turn might be due to chance or a mundane reason, such as is the case with the rule of the road and side of the steering wheel).3 If the latter is true, active steps could be considered to intervene in medical curricula in such a way to accommodate the bias. Moreover, given that it was shown that surgical results for paired organs differ depending on the laterality of pathology, it is plausible that the same might hold true for neurosurgical procedures.2 In this respect it would be worthwhile investigating whether there are differences in outcomes in surgery of brain regions with regard to the side of the lesion (adjusted for eloquence). If such a difference exists and is concordant with the bias in neurosurgical visualization (i.e. right sided craniotomies have better outcomes than left sided), it gives ground to an effort to correct the bias.
It is worth noticing that the same fact – being close to midline – enables bilateral depictions, whereas entities away from the midline preclude such depictions. Indeed, all interlaminectomy and most lumbar disc herniation depictions we included in the analysis showed both sides, whereas all pterional craniotomies and most retromastoid craniotomies were shown on exclusively right side, with the contralateral side not being depicted. Even though this explains the lack of contralateral representation in the medical images, it does not however explain the significant bias toward the right side in visualization and depiction.
Our results show a clear bias in how pathology is represented in the medical literature (Table 2). An interesting and important question to be investigated in the future is whether this bias might affect wrong-side surgery, which is a known and serious problem.14–17 It merits a research effort to determine whether accommodating the bias could be associated with the incidence of wrong-side surgery and whether there is also laterality bias in the wrong-side neurosurgical procedures. If the association indeed exists, correcting the bias (e.g. via an intervention into the medical textbooks, or guideline proposal for neurosurgical journals) might be a practical and inexpensive way to reduce the incidence of wrong-side procedures.
There are limitations to our research, the major due to sampling. Namely, we recruited a convenient sample which might not be representative of the general neurosurgical population. Second, the sample size was inadequate to analyze associations between sociodemographic variables and lateralization. Nevertheless, we believe that the main findings are robust enough to warrant an informed discussion, without the need for secondary analysis. Third, the real-life implications of the investigated phenomenon are unknown, as we did not research any association with execution of surgical maneuvers, or patient outcomes.
ConclusionThe mixture of choices with regard to laterality in imagining and depicting neurosurgical anatomy is not racemic. There is a significant bias among neurosurgeons in laterality in processing topographical information on anatomy and pathology. It remains to be researched whether this phenomenon translates into decision making and treatment outcomes, what the underlying causes are, and whether they are modifiable.
FundingHrvoje Barić is the 2024 Helsinki C. Ehrnrooth Clinical Vascular and Skull Base Fellow.
The following is Supplementary data to this article: