









To describe pros and cons of some radiation protection measures and the implications on the design of a neurosurgery operating room.
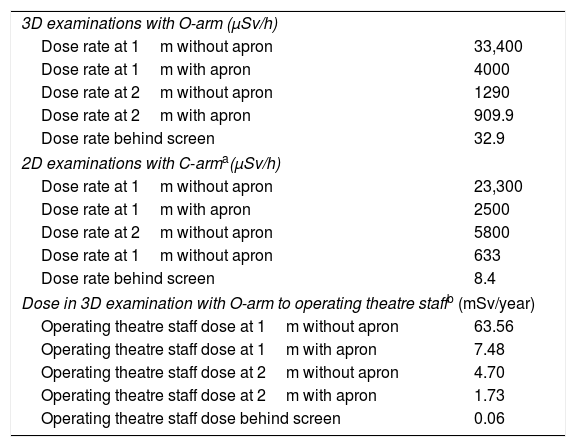
Material and methodsConcurring with the acquisition and use of an O-arm device, a structural remodelling of our neurosurgery operating room was carried out. The theatre was enlarged, the shielding was reinforced and a foldable leaded screen was installed inside the operating room. Radiation doses were measured in front of and behind the screen.
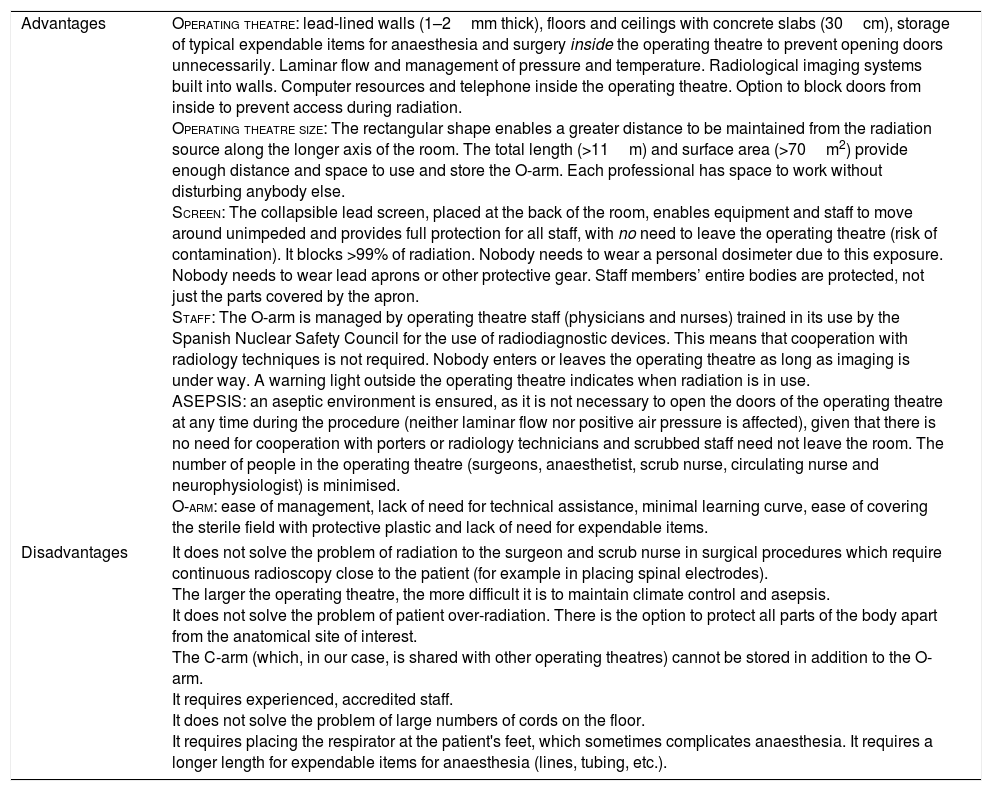
ResultsThe screen provides whole-body radiation protection for all the personnel inside the theatre (effective dose <5μSv at 2.5m from the gantry per O-arm exploration; 0.0μSv received behind the screen per O-arm exploration; and undetectable cumulative annual radiation dose behind the screen), obviates the need for leaded aprons and personal dosimeters, and minimises the circulation of personnel. Enlarging the size of the operating room allows storing the equipment inside and minimises the risk of collision and contamination. Rectangular rooms provide greater distance from the source of radiation.
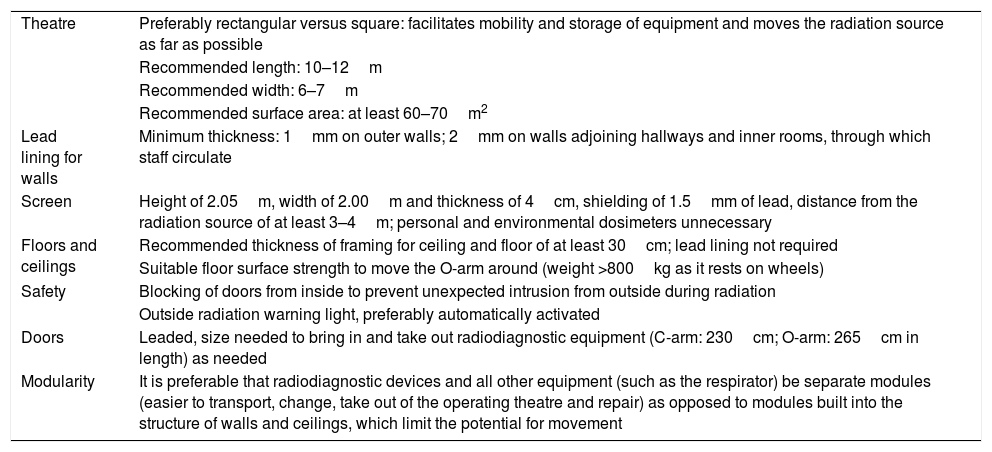
ConclusionFloor, ceiling and walls shielding, a rectangular-shaped and large enough theatre, the presence of a foldable leaded screen, and the security systems precluding an unexpected irruption into the operating room during irradiation are relevant issues to consider when designing a neurosurgery operating theatre.
Describir pros y contras de diversas medidas de protección radiológica y sus implicaciones en el diseño de un quirófano de neurocirugía.
Material y métodosSe realizó una reforma estructural del quirófano de neurocirugía a propósito de la adquisición y uso de un O-arm. Se ampliaron las medidas y blindajes del quirófano, y se instaló una mampara blindada y abatible en su interior. Se midieron dosis de radiación delante y detrás de la mampara.
ResultadosLa mampara proporciona una radioprotección integral para todo el personal de quirófano (dosis<5μSv a 2,5 m del gantry por cada exploración con O-arm; 0,0μSv tras la mampara por cada exploración de O-arm; dosis acumulada anual tras la mampara, indetectable), obvia la necesidad de delantales plomados y dosímetros personales y minimiza la circulación de personal. El aumento del tamaño del quirófano permite almacenar los equipos dentro y minimiza el riesgo de colisión o contaminación. Los quirófanos rectangulares permiten aumentar la distancia al foco emisor de radiación.
ConclusionesEl blindaje de paredes, techos y suelos, la forma rectangular y la superficie lo más amplia posible, la presencia de una mampara plomada y abatible, y los sistemas de seguridad que impiden una irrupción inesperada en el quirófano mientras se está irradiando son cuestiones relevantes a tener en cuenta en el diseño del quirófano de neurocirugía.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



