

P-005 - CENTRAL SKULL BASE MUCORMYCOSIS: ATYPICAL PRESENTATION AND MANAGEMENT ISSUES
Complejo Hospitalario Universitario de Albacete, Albacete, España.
Introduction: Mucormycosis (MCR) is an acute, fulminant, and often lethal opportunistic infection principally diagnosed in patients with underlying comorbidities, such as diabetes mellitus or immunocompromised status. Central skull base osteomyelitis secondary to a rhinoorbitocerebral form of infection is a rare presentation because of the angio-invasive characteristic of Mucor. Due to the broad range of signs and symptoms that can appear (headache, cranial neuropathies...) and the nonspecific radiologic findings and laboratory tests, diagnosis is often delayed. Regularly, a biopsy is required for histopathological confirmation. MCR can cause extensive progression, leading to high morbidity and mortality.
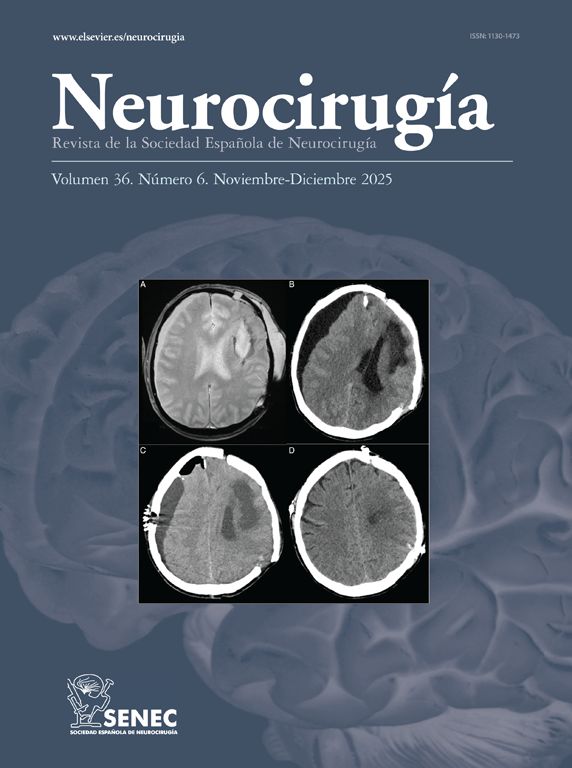
Case report: A 51-year-old male with a past medical history of type two diabetes mellitus, hypertension, hyperlipidemia, and obesity, presented with a chronic headache and facial pain with no improvement after medical treatment. Initial diagnosis was sinusitis with neuralgia of the sphenopalatine nerve. Laboratory tests showed panhypopituitarism. CT scan revealed pansinusitis and lytic lesions in the sphenoid bone and skull base. MRI was performed showing a preclival and sellar mass-like soft tissue hypointense on T1WI with invasion of the cavernous sinus and left orbit. After contrast, heterogeneous enhancing lesion of the sellar and para sellar location was observed. Biopsy of the clivus and hypophysis was performed via transsphenoidal approach. Culture test was positive for MCR. Emergency endoscopic debridement involving all sinus was done, which showed necrotic lesions in the nasopharynx. Postoperatively, treatment with amphotericin B250 followed by Posaconazole was administered. After 6 months, the patient is asymptomatic.
Discussion: MCR is an angio-invasive organism extending infection through perivascular channels, causing infarction, thrombosis or vasculitis, necrosis of the tissue, and systemic dissemination. Rapid diagnosis is required because of the high morbidity and mortality of this entity. Multidisciplinary treatment for these patients encompasses surgical debridement and post-op anti-fungal treatment.



