






To evaluate both the short-term and long-term outcomes of odontoid screw fixation (OSF), identifying potential risk factors for implant-related complications in patients with odontoid fractures.
MethodsThis is a retrospective observational cohort study. Inclusion criteria were as follows: 1) Type II fractures and rostral Type III fractures, according to the Anderson and D’Alonzo classification; 2) patients older than 15 years. Exclusion criteria were: 1) other Type III injuries; 2) osteoporosis confirmed by densitometry or a CT bone density score below 100 Hounsfield units; 3) odontoid fractures related to tumors or aneurysmal bone cysts.
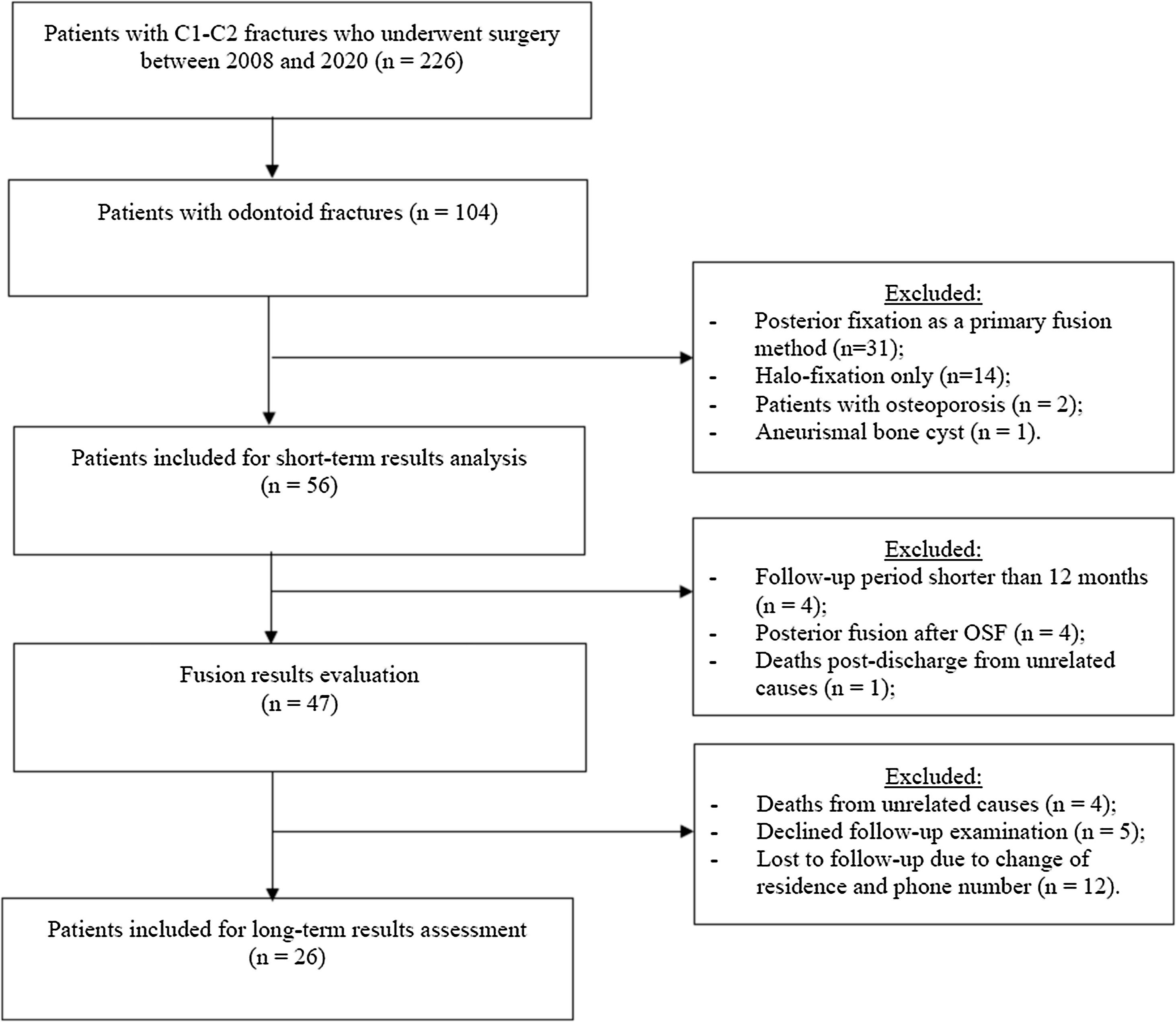
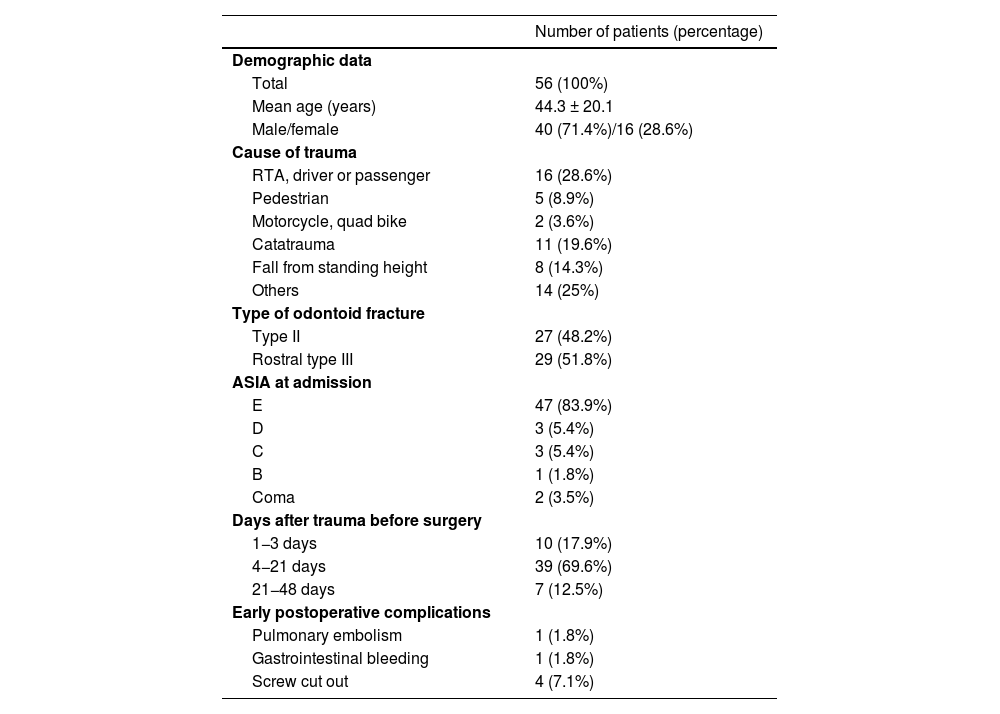
ResultsIn total, 56 patients were considered for the analysis of short-term results, and 26 patients were evaluated for long-term outcomes. No significant differences were observed in the preoperative imaging data and intraoperative features of OSF between patients with Type II and rostral Type III fractures. The mean operative duration was 63.9 ± 20.9 min, and the mean intraoperative blood loss was 22.1 ± 22.9 ml.
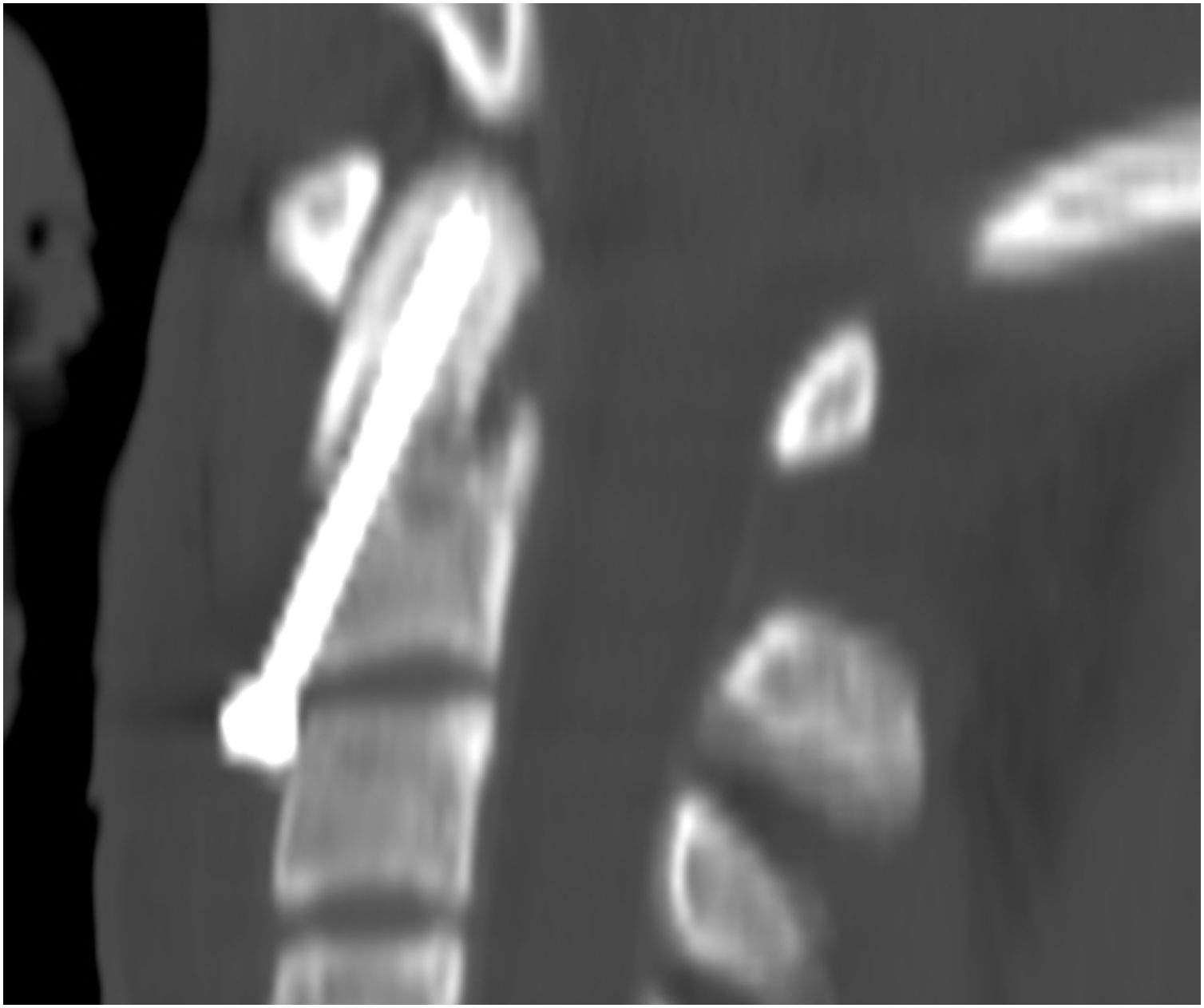
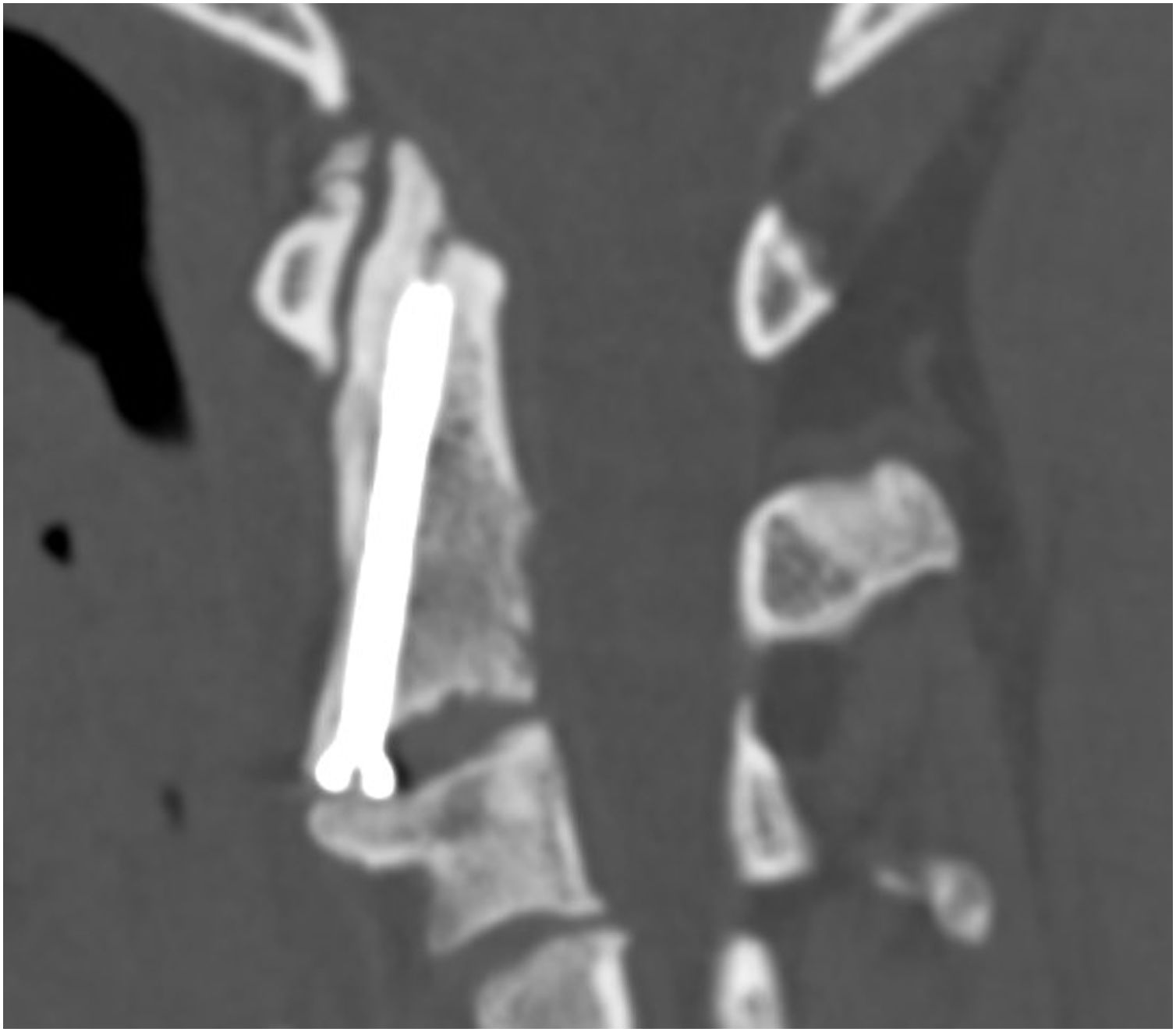
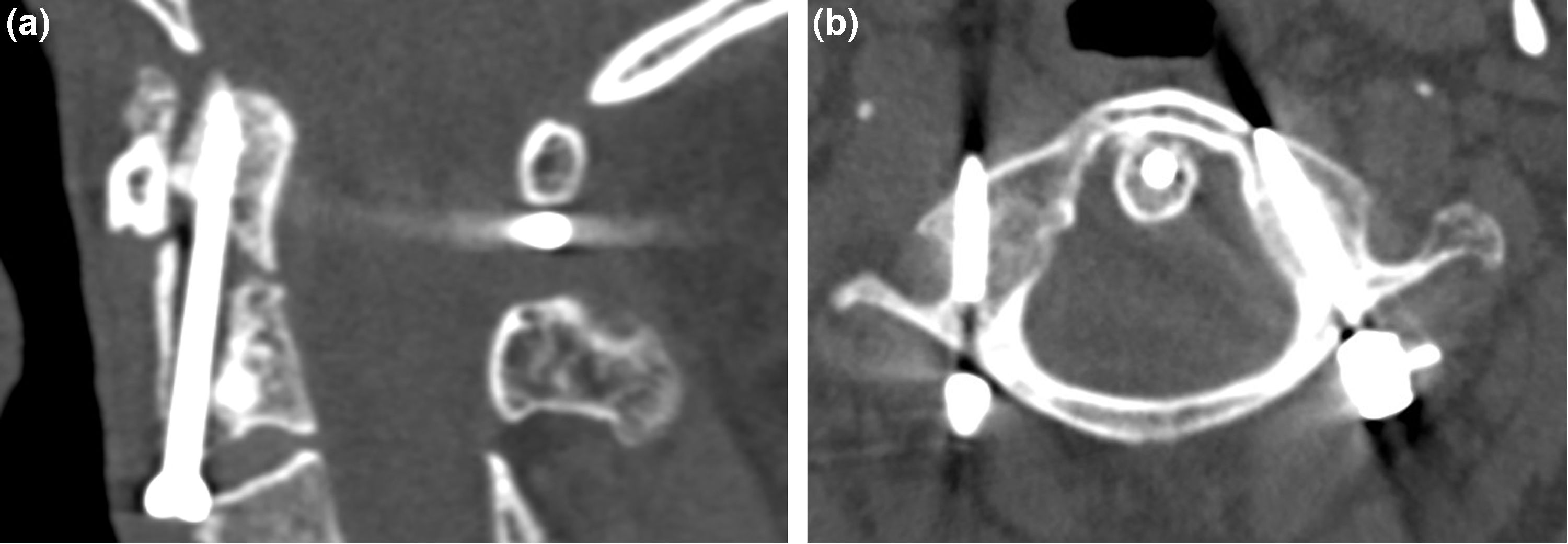
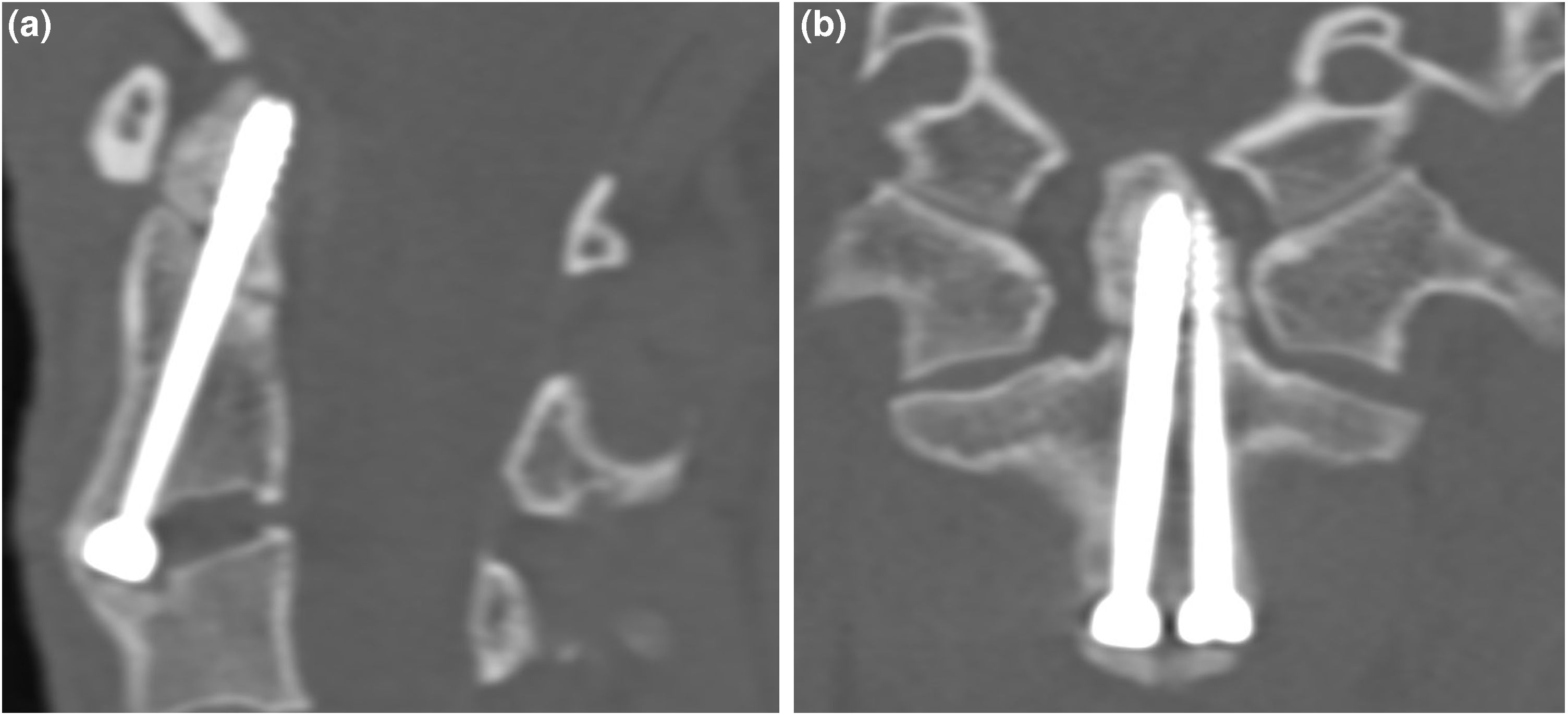
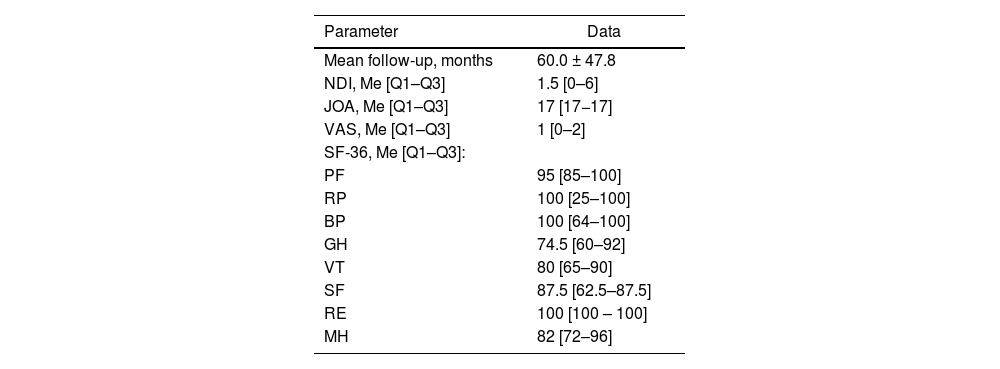
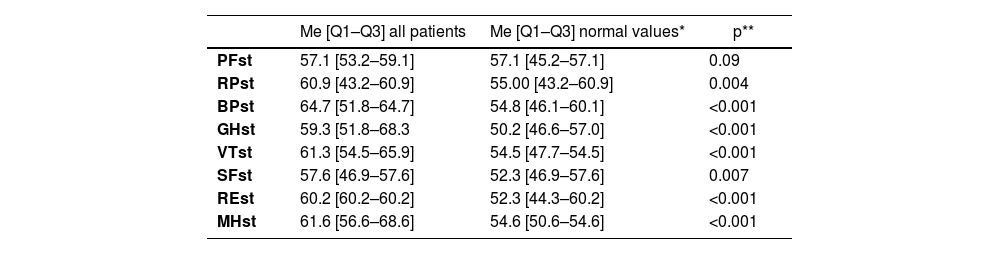
Screw cut-out was identified in four patients with rostral Type III fractures (p = 0.04). The rate of screw cut-out was found to correlate with the degree of dens fragment displacement. The bone fusion rate was 95.7%. CT scans identified stable pseudarthrosis in two cases. We observed C2–C3 ankylosis in all cases following partial disc resection. One third of patients with screws placed through the anterior lip of C2 showed no C2–C3 ankylosis. A strong trend towards lateral joint ankylosis formation in patients with a median lateral mass dislocation of 11.9 mm was observed. Most SF-36 scores either matched or exceeded the corresponding normal median values in the published reference database.
ConclusionsOSF is a reliable treatment method of Type II and rostral Type III odontoid fractures with fragment displacement of 4 mm or less. The minimally invasive OSF through the anterior-inferior lip of C2, using monocortical screw placement and cannulated instruments, without rigid intraoperative head immobilization, is sufficient to achieve favorable clinical and fusion results. This technique reduces the risk of ankylosis in the C2–C3 segment. OSF restore the quality of life for patients with odontoid fractures to levels comparable to those of the general population norm.
Evaluar tanto los resultados a corto como a largo plazo de la fijación con tornillo del odontoide (OSF), identificando posibles factores de riesgo para complicaciones relacionadas con el implante en pacientes con fracturas odontoides.
MétodosEste es un estudio de cohorte observacional retrospectivo. Los criterios de inclusión fueron los siguientes: 1) fracturas Tipo II y fracturas Tipo III rostral, según la clasificación de Anderson y D’Alonzo; 2) pacientes mayores de 15 años. Los criterios de exclusión fueron: 1) otras lesiones Tipo III; 2) osteoporosis confirmada por densitometría o una puntuación de densidad ósea en CT por debajo de 100 unidades Hounsfield; 3) fracturas odontoides relacionadas con tumores o quistes óseos aneurismáticos.
ResultadosEn total, 56 pacientes fueron considerados para el análisis de resultados a corto plazo, y 26 pacientes fueron evaluados para resultados a largo plazo. No se observaron diferencias significativas en los datos de imagen preoperatoria y características intraoperatorias de la OSF entre pacientes con fracturas Tipo II y Tipo III rostral. La duración media de la operación fue de 63,9 ± 20,9 minutos, y la pérdida media de sangre intraoperatoria fue de 22,1 ± 22,9 ml.
El desplazamiento del tornillo se identificó en cuatro pacientes con fracturas Tipo III rostral (p = 0.04). Se encontró que la tasa de desplazamiento del tornillo estaba correlacionada con el grado de desplazamiento del fragmento del dens. La tasa de fusión ósea fue del 95.7%. Las tomografías computarizadas identificaron pseudartrosis estables en dos casos. Observamos anquilosis C2–C3 en todos los casos tras la resección parcial del disco. Un tercio de los pacientes con tornillos colocados a través del labio anterior de C2 no mostraron anquilosis C2–C3. Se observó una fuerte tendencia hacia la formación de anquilosis de la articulación lateral en pacientes con una dislocación lateral media de la masa de 11,9 mm. La mayoría de las puntuaciones SF-36 coincidieron o superaron los valores medianos normales correspondientes en la base de datos de referencia publicada.
ConclusionesLa OSF es un método de tratamiento confiable para fracturas odontoides de tipo II y tipo III rostral con desplazamiento del fragmento de 4 mm o menos. La OSF mínimamente invasiva a través del labio anteroinferior de C2, utilizando colocación de tornillo monocortical e instrumentos canulados, sin inmovilización rígida intraoperatoria de la cabeza, es suficiente para lograr resultados clínicos y de fusión favorables. Esta técnica reduce el riesgo de anquilosis en el segmento C2-C3. La OSF restaura la calidad de vida de los pacientes con fracturas odontoides a niveles comparables a los de la norma de la población general.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.