






Acute presentation with intracranial hemorrhage owing to a previously silent brain tumor (BT) is rare. Although any BT can bleed, the frequency and type of bleeding varies across tumor types.
Materials and methodsWe aimed to retrospectively review our experience with 55 patients with BTs presenting with ICH.
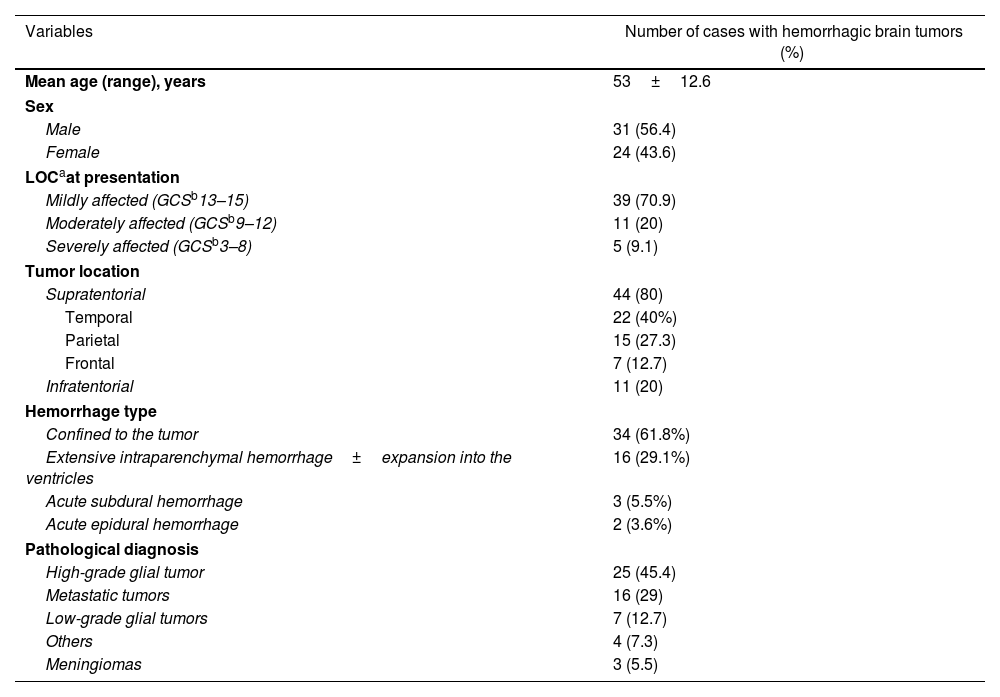
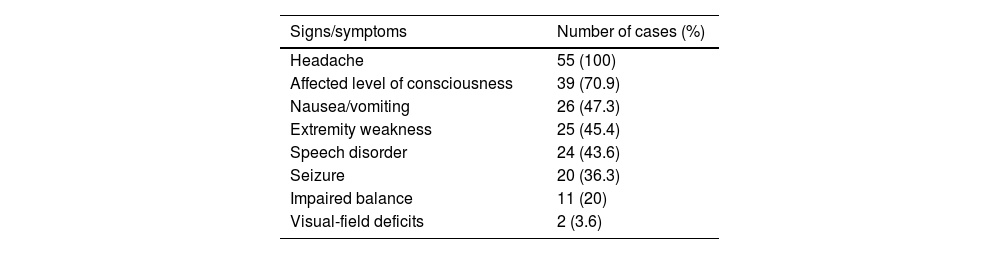
ResultsSigns of increased intracranial pressure were the most common symptoms. The temporal lobe was the most common lesion site (n=22). Hemorrhages were mainly confined to the tumor margins (HCTs) (n=34). Extensive intraparenchymal hemorrhages (EIHs) were mainly associated with moderately/severely decreased levels of consciousness (LOCs) (n=15/16). High-grade glioma (HGGT) (n=25) was the leading pathological diagnosis followed by metastasis (MBT) (n=16/55). The hemorrhage type was associated with the pathological diagnosis of the tumor. Patients with HGGT (n=19/25) and MBT (n=9/16) mainly presented with HCTs, whereas low-grade gliomas (LGGT) primarily caused EIHs (n=6/7).
ConclusionsHemorrhagic presentation is a rare occurrence in BTs. Among all, MBT and HGGT are responsible for majority of the cases. Importantly, despite their relatively benign characteristics, LGGTs mainly result in extensive parenchymal destruction once they bleed. Maximum surgical resection of hemorrhagic BTs and decompression of the affected brain regions followed by histological confirmation of the diagnosis should be the main goals of treatment in cases with hemorrhagic BTs.
La presentación aguda con hemorragia intracraneal debida a un tumor cerebral (BT) anteriormente silencioso es rara. A pesar de que cualquier BT puede sangrar, la frecuencia y el tipo de sangrado varían según el tipo de tumor.
Materiales y métodosNuestro objetivo fue reexaminar retrospectivamente nuestra experiencia con 55 pacientes con los BT que presentaban HIC.
ResultadosLos síntomas más comunes fueron signos de aumento de la presión intracraneal. El lóbulo temporal fue el sitio de lesión más común (n=22). Las hemorragias se limitaron especialmente a los márgenes tumorales (HCT) (n=34). Las hemorragias intraparenquimatosas extensas (HIE) se asociaron mayormente con niveles de conciencia moderada/severamente disminuidos (LOC) (n=15/16). El glioma de alto grado (HGGT) (n=25) fue el principal diagnóstico patológico después de la metástasis (MBT) (n=16/55). El tipo de hemorragia se asoció con el diagnóstico patológico del tumor. Los pacientes con HGGT (n=19/25) y MBT (n=9/16) presentaron mayormente con HCT, mientras que los gliomas de bajo grado (LGGT) causaron principalmente HIE (n=6/7).
ConclusionesLa presentación hemorrágica es una ocurrencia rara en los BT. Entre todos, MBT y HGGT son responsables de la mayoría de los casos. Más importante aún, pese a sus características relativamente benignas, los LGGT resultan mayormente una destrucción extensa del parénquima una vez que sangran. La resección quirúrgica máxima de BT hemorrágicos y la descompresión de las regiones cerebrales afectadas con la confirmación histológica del diagnóstico deben ser los objetivos principales del tratamiento en casos con BT hemorrágicos.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



