


Aneurysmal subarachnoid hemorrhage is an urgent manner in which blood accumulates in the subarachnoid region. Presence of chronic kidney disease (CKD) is often a predictor of adverse outcomes perioperatively. Patients with CKD may have different perioperative outcomes during surgery for aneurysmal subarachnoid hemorrhage compared to patients without CKD, and we sought to retrospectively examine the effect of CKD on perioperative outcomes in aSAH patients receiving surgery.
MethodsPatients undergoing craniotomy for aneurysmal subarachnoid hemorrhage were analyzed using the ACS-NSQIP database from 2005 to 2021. Patients with CKD were defined based on estimated glomerular filtration rate (eGFR) <60mL/min. 30-Day postoperative outcomes were compared between the two groups and included death, cardiac complications, renal complications, sepsis, pulmonary complications, return to the operating room (OR), and operation time greater than 4h, among other variables.
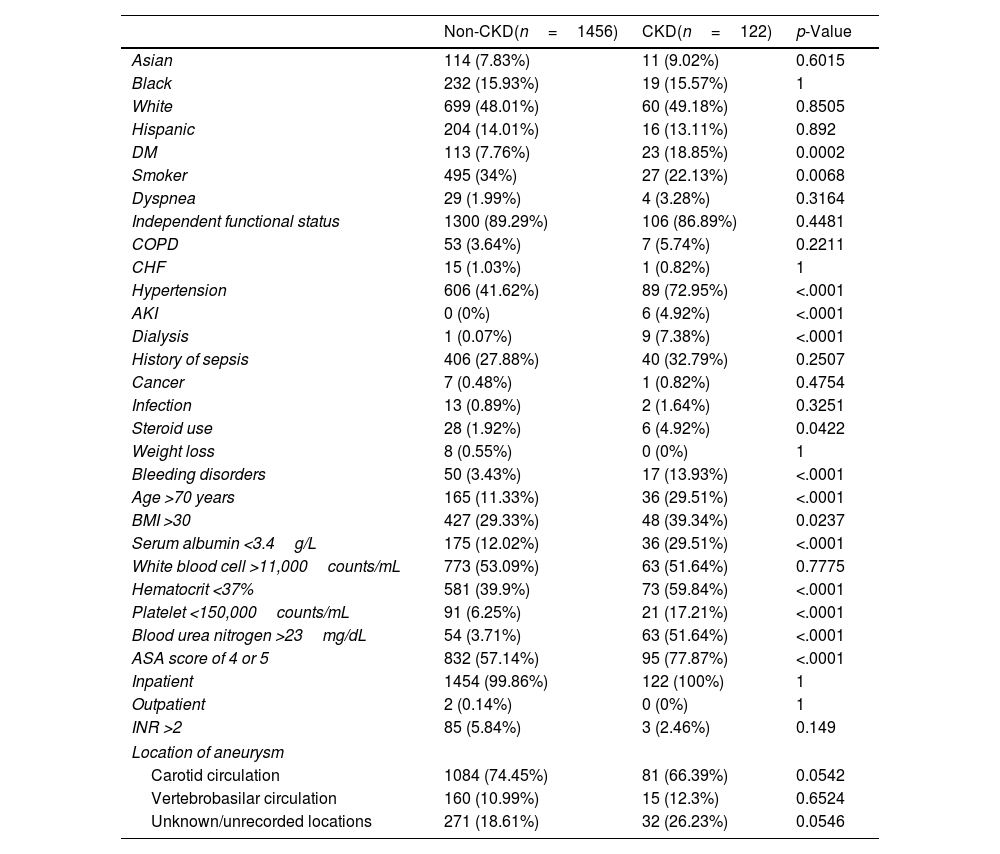
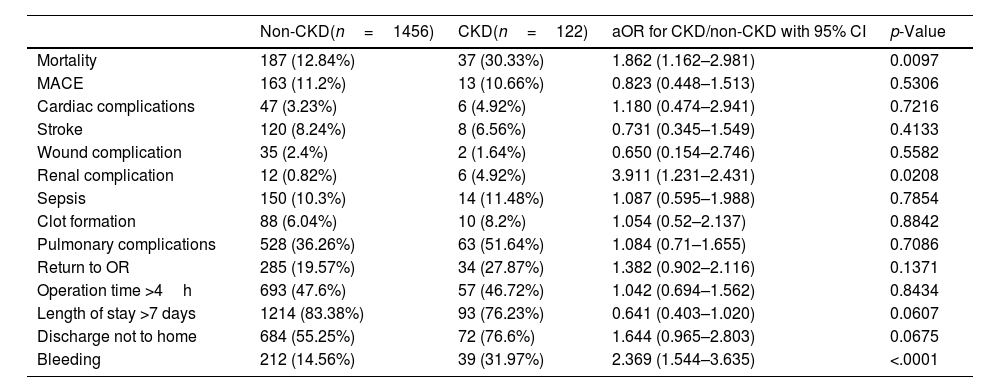
ResultsThere were 122 CKD patients and 1456 non-CKD aSAH patients who underwent craniotomy identified. Compared to non-CKD patients, CKD patients had increased risk of mortality (30.33% vs. 12.84%, aOR 1.862, p=0.0097), renal complications (4.92% vs. 0.82%, aOR 3.911, p=0.0208), and bleeding perioperatively (31.97% vs. 14.56%, aOR 2.369, p<0.0001).
ConclusionThis study demonstrated that CKD patients with aneurysmal subarachnoid hemorrhage receiving craniotomy have increased risk of death, renal complications, and bleeding perioperatively.
La hemorragia subaracnoidea aneurismática es una urgencia médica caracterizada por la acumulación de sangre en el espacio subaracnoideo. La presencia de enfermedad renal crónica (ERC) suele ser un predictor de resultados adversos en el período perioperatorio. Los pacientes con ERC pueden presentar desenlaces perioperatorios diferentes durante la cirugía por hemorragia subaracnoidea aneurismática en comparación con los pacientes sin ERC, por lo que buscamos examinar retrospectivamente el efecto de la ERC en los resultados perioperatorios de pacientes con HSA aneurismática sometidos a cirugía.
MétodosSe analizaron pacientes sometidos a craneotomía por hemorragia subaracnoidea aneurismática utilizando la base de datos ACS-NSQIP entre 2005 y 2021. Los pacientes con ERC se definieron como aquellos con una tasa de filtración glomerular estimada (TFGe) <60mL/min. Se compararon los resultados postoperatorios a 30 días entre ambos grupos, incluyendo mortalidad, complicaciones cardíacas, complicaciones renales, sepsis, complicaciones pulmonares, retorno a quirófano y tiempo operatorio mayor de cuatro horas, entre otras variables.
ResultadosSe identificaron 122 pacientes con ERC y 1,456 pacientes sin ERC sometidos a craneotomía por HSA. En comparación con los pacientes sin ERC, los pacientes con ERC presentaron un mayor riesgo de mortalidad (30.33% vs. 12.84%, ORa 1.862, p=0.0097), complicaciones renales (4.92% vs. 0.82%, ORa 3.911, p=0.0208) y sangrado perioperatorio (31.97% vs. 14.56%, ORa 2.369, p<0.0001).
ConclusiónEste estudio demuestra que los pacientes con enfermedad renal crónica sometidos a craneotomía por hemorragia subaracnoidea aneurismática presentan un mayor riesgo de muerte, complicaciones renales y sangrado en el período perioperatorio.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



