








Meningiomas associating prominent cystic changes (CM) have challenged neurosurgeons since the beginning of this surgical discipline. We present the experience in the diagnostic and therapeutic management of this entity in our institution.
Material and methodsA review of our patient database was carried out, searching for those CM that were operated on in the last 15 years. Relevant clinical data were recorded and analysed for each case, with special emphasis in the correlation of radiological and pathological findings. Cystic changes were classified according to the scheme proposed by Nauta et al.
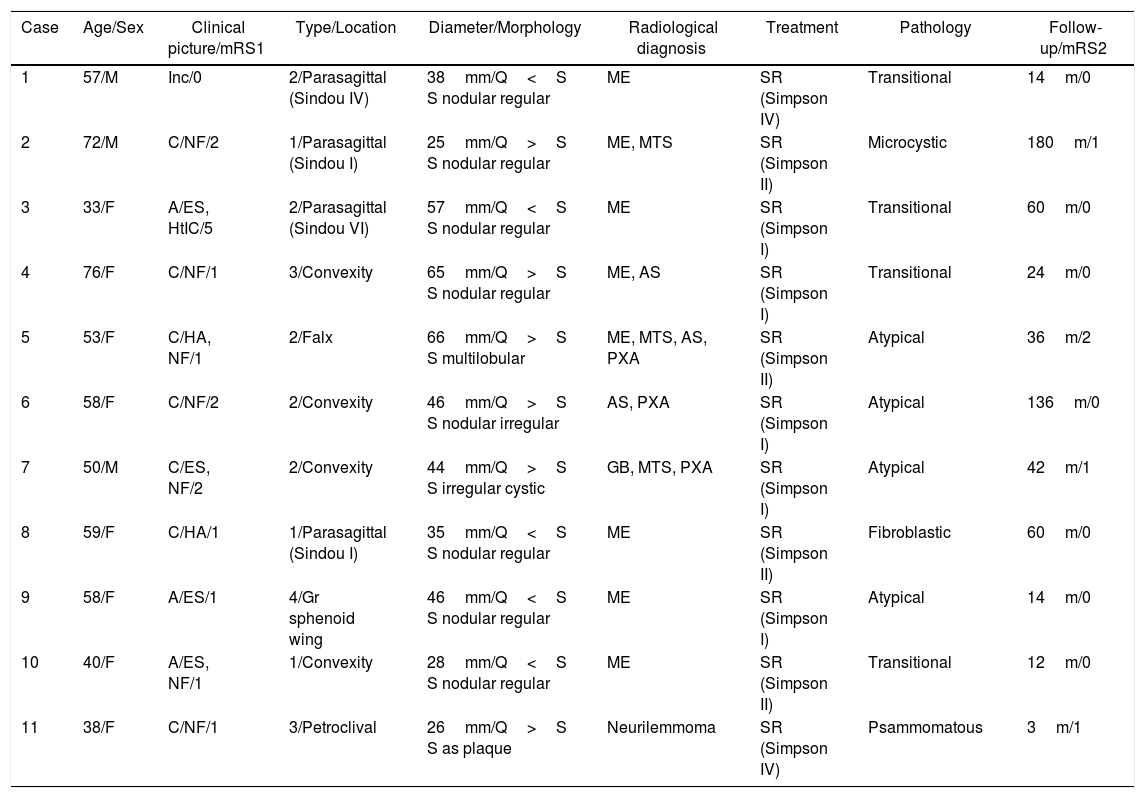
ResultsA total of 11 patients were gathered, which represents 1.8% of the meningiomas operated on in our department during the period studied. All were adults, predominantly female patients (8 cases). Among the clinical symptoms a high rate of epileptic seizures was observed while only one patient developed acute intracranial hypertension. Morphologically, most tumours corresponded to type 2 CMs, followed by types 1, 3 and 4. In only five patients an unequivocal radiological diagnosis of meningioma could be made. All neoplasms were surgically removed and there were no records of recurrence (mean follow-up: 52.8 months). Microscopic findings were consistent with the pathological diagnosis of atypical meningioma in 4 cases, while the remaining tumours corresponded to OMS grade I neoplasms with variable microscopic patterns.
ConclusionsMeningiomas can exceptionally associate cystic changes, both intra and/or extratumoral, in variable number and size. When cystic changes become too prominent (a large number or big-sized cysts), a serious preoperative diagnostic dilemma may arise. The surgical management of those CMs displaying a peripheral, thin-walled cyst (types 2 and 3) is especially complex, as contrast enhancement of the tumour wall did not correlate strictly with neoplastic invasion; even in the absence of this feature free floating islands of meningothelial cells intermixed with cyst fluid can be found.
Consequently both surgical biopsy of every suspicious tissue and copious irrigation of the surgical cavity are strongly recommended for these CM types.
Los meningiomas que asocian cambios quísticos prominentes (MQ) han representado un reto diagnóstico y terapéutico desde los orígenes de la neurocirugía moderna. Presentamos la experiencia en el manejo clínico y quirúrgico de esta entidad en nuestro Servicio.
Material y métodosEn este estudio descriptivo se incluyen los MQ intervenidos en nuestro Servicio en los últimos 15 años, evaluando las variables clínicas, diagnósticas y terapéuticas de este subgrupo de meningiomas, con especial énfasis en la correlación de los hallazgos radiológicos y patológicos. Los tumores se clasificaron siguiendo el esquema propuesto por Nauta y sus colaboradores.
ResultadosSe identificaron 11 casos, lo que supone un 1,8% de los meningiomas intervenidos en ese periodo. Todos los pacientes eran adultos y 8 de ellos, mujeres. Entre los síntomas, destacó la alta frecuencia de crisis epilépticas, mientras que solo un caso desarrolló hipertensión intracraneal aguda. La morfología predominante fue el tipo 2, seguida de los tipos 1, 3 y 4. En 5 casos pudo establecerse un diagnóstico radiológico inequívoco de meningioma. Todos los pacientes fueron tratados mediante cirugía, sin evidenciarse casos de recurrencia durante un seguimiento medio de 52,8 meses. Aunque la mayoría de las neoplasias correspondieron al grado i de la OMS, incluyendo subtipos variados, 4 de ellas fueron diagnosticadas como meningiomas atípicos.
ConclusionesDe forma excepcional, los meningiomas pueden desarrollar cambios quísticos, intra- o extratumorales, en número y tamaño variable. Estos constituyen hallazgos poco típicos que pueden dificultar seriamente su diagnóstico diferencial radiológico. Los meningiomas con quistes periféricos de cápsula fina (tipos 2 y 3) suponen el escenario quirúrgico más complejo, pues el realce capsular en las pruebas de imagen no traduce necesariamente infiltración tumoral, mientras que el quiste puede contener células neoplásicas. Por lo tanto, recomendamos realizar al menos biopsia de la cápsula o seudocápsula, y lavado minucioso de la cavidad quirúrgica especialmente en estos subtipos.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



